Recently, this very topic has come up very often on our portal - analysis of different tumor markers. Today we will have a whole selection for diagnosing a group of diseases. We will talk about the work of the gastrointestinal tract as a whole. So let’s look at the intestinal tumor markers step by step, with feeling, clearly, and in order. We will find out what they are, how they do them, what results should be - in general, we will delve into this topic headlong to the delight of our reader.
Let us note that tumor markers are only one of the possible first ways to examine an emerging disease. Some markers are indeed capable of indicating the presence of a tumor with a high probability, but one way or another, the final diagnosis for making a correct diagnosis is already done by other means. In the meantime, we are returning to donating our blood.
Studying the results of the general analysis
Normally, the amount of hemoglobin as the main component of red blood cells is 120-150 g/l in women and 130-170 g/l in men. In case of tumor development, its decrease to 128 g/l is observed.
The number of white blood cells, which protect the body from toxins, dying cells, viruses and bacteria, in a cancer patient is several times higher than normal. A general blood test allows you to determine the number of platelets, indicating the development of cancer.
Rectal cancer causes an increase in the number of leukocytes in patients in the second stage of the process to 8-9 thousand/mm³, and in some cases hyperleukocytosis is observed - 40-50 thousand/mm³. The total number of young cells gradually increases. The erythrocyte sedimentation rate (ESR) reaches high levels, and even after a course of treatment, high levels persist for a long time.
Normally, ESR in a healthy person is 1-15 mm/h. If the rectum is involved in the tumor process, the erythrocyte sedimentation rate reaches critical figures - 60-70 mm/h. Additional research is necessary if high levels of not only ESR, but also hemoglobin are detected.
Interpretation of results
For patients with rectal cancer, determining the dynamics of disease development and the effectiveness of therapy depends on the level of CEA concentration in the blood. An increase in antigen levels indicates that the disease is progressing. If this marker tends to decrease, the therapy has a positive effect. The CEA tumor marker makes it possible to detect relapse of the disease after completing a course of treatment. Already in the initial stages of cancer, when the first symptoms are absent, the concentration of antigen in the blood increases significantly. With the development of a malignant tumor of the rectum, the symptoms intensify, and the CEA marker continues to increase.
This marker may indicate not only rectal cancer, but also the presence of other cancers. It is used as a marker to detect oncology of the gastrointestinal tract, as well as lung cancer. An increase in antigen levels can also be caused by autoimmune or chronic diseases, as well as bad habits (smoking). Therefore, if symptoms characteristic of a cancerous tumor do not appear, a definitive diagnosis is not recommended.
Education:
Graduated from the Russian National Research Medical University. N.I. Pirogov, Faculty of Medicine. Took advanced training courses. Primary specialization is in coloproctology at the State Scientific Center for Coloproctology. Worked at the City Scientific and Practical Center for Coloproctology of St. Petersburg.
Experience:
Proctologist. Medical practice experience – 25 years. Author of more than 40 articles on medical topics. A regular participant in conferences and symposia, where problems of modern medicine are covered.
Provides highly qualified diagnosis and treatment of many diseases: hemorrhoids, anal fissures, various diseases of the colon, and successfully diagnoses neoplasms of the perianal area and rectum in the early stages. Also conducts examinations of children.
Tumor markers
- these are substances that are produced by neoplasm cells or nearby cells. To diagnose and monitor the effectiveness of treatment of malignant intestinal tumors, an immunological study is performed to identify tumor markers. Their concentration is influenced by the aggressiveness of tumor growth and the extent of the process, which makes it possible to suspect cancer and evaluate the effectiveness of therapy, and determine the degree of radical intervention.
Over 200 tumor markers have been identified, but approximately 20 types are identified in clinical practice. Among them are:
- specific markers that most likely indicate a malignant process in a specific location (for example, in the intestine);
- nonspecific markers indicating the presence of malignancy, regardless of its location, or having low sensitivity for intestinal cancer.
To judge the prevalence of the process and the effectiveness of treatment, the concentration of both tumor markers is determined.
Specific
There are no ideal markers that accurately indicate the presence of a malignant tumor in the intestine. The most sensitive ones are:
- Carcinoembryonic antigen (CEA). It belongs to the class of oncofetal markers. Normally, it is produced in the fetus in the stomach and intestines. After birth, CEA production decreases. Its concentration increases significantly in colorectal cancer.
- CA 19-9. This glycoprotein is found in the fetal epithelium of the intestines, stomach, and pancreas. This tumor marker is less specific. Its concentration increases significantly in pancreatic cancer and cholestasis.
- CA 72-4. Its level rarely increases in inflammatory diseases and increases significantly in cancer of the stomach and intestines.
- Tumor-M2-pyruvate kinase (Tu M2-PK). The enzyme is produced in the gastrointestinal tract by proliferating malignant cells. Has 70% specificity for colorectal cancer. Its concentration depends on the stage of the disease. The main feature is that this tumor marker is determined not only in the blood, but also in the feces.
To identify the extent of the process and the presence of metastases, an immunological study of nonspecific tumor growth markers is performed.
Assessing the level of tumor markers in the primary diagnosis of colon cancer is not always justified. The values of tumor markers are not always directly related to the disease being diagnosed. An increase in the indicator may have nothing to do with bowel cancer. Conversely, a low level of a tumor marker does not guarantee the absence of a malignant tumor. An accurate diagnosis can only be made after a complete examination by a specialized specialist.
In oncology, tumor markers are used primarily to monitor the patient's condition. If during the initial examination the patient had a high level of a tumor marker, its growth is subsequently monitored. After the tumor is removed, its concentration in the blood decreases sharply. Repeated growth of the tumor marker indicates tumor recurrence.
Nonspecific
Nonspecific tumor markers of intestinal cancer include those substances whose concentration rarely increases in this disease, and those that increase in any type of tumor:
A referral for tumor marker testing is given by an oncologist
. It is the doctor who determines which of the specific and nonspecific indicators of malignant formations are important for diagnosing intestinal cancer and differentiating the disease from benign diseases.
Specific proteins: early diagnosis
A blood test is performed to determine the presence of tumor markers in the blood. Special proteins produced by tumor cells can significantly exceed normal levels.
The following markers are used to detect cancer in the intestine:
- REA;
- CA 19-9;
- CA 242;
- CA 72-4.
The main specific proteins found in the patient’s blood make it possible to predict the development of a relapse of the disease even before the onset of the first symptoms. If tumor markers are identified, the patient must undergo a comprehensive examination to determine the location of the cancer tumor.
Special proteins contain 200 compounds, but only specific markers are needed to diagnose colon cancer. The tumor research algorithm includes the use of CEA and CA 19, but the leading role in determining cancer of the bile ducts and rectum belongs to CA 19.
The level of tumor markers in the patient’s blood is influenced by the following factors:
- serum storage conditions;
- tumor mass;
- mechanism of blood supply to cancerous tissues;
- metabolism in cells.
When is analysis needed?
Not so long ago, it was possible to determine the development of a malignant tumor in the intestine at the initial stage only by conducting a diagnostic examination regarding another pathological condition. To detect cancer of the digestive system, specialists prescribe a blood test for intestinal cancer to detect certain tumor markers.
On this topic
- Oncogastroenterology
Feces for stomach cancer
- Natalya Gennadievna Butsyk
- December 6, 2020
Laboratory research is carried out if there are such signs as:
- rapid weight loss;
- weakness;
- increased fatigue ;
- decreased or absent desire to eat .
In addition, a procedure to identify tumor markers of the stomach and intestines is carried out if there is an assumption of the development of oncopathology of the colon and rectum. The analysis is also necessary to assess how effective the prescribed treatment was and to predict the likelihood of recurrence of the disease during remission.
Such blood indicators, as a rule, indicate the presence of a malignant lesion, the localization of the tumor, and the degree of its spread.
Examination for a malignant tumor in the intestine
The following symptoms should alert the patient and serve as an indication for a blood test:
- stomach bleeding;
- constipation;
- urinary incontinence;
- flatulence;
- abdominal pain.
Tests for bowel cancer are necessary to confirm the diagnosis. Blood testing is carried out in the morning, and in emergency cases - at any time. Blood sampling must be carried out at the same time, since changes may occur during the day.
In the process of studying the material, the reasons for the increase or decrease in hemoglobin, leukocytes, platelets are determined and the ESR (erythrocyte sedimentation rate) is determined. A thorough study of peripheral blood parameters is carried out, comparing them with normal values in a healthy person. In addition, certain information is provided by studying the average volume of red blood cells and the total amount of hemoglobin, the value of the color index, the presence of eosinophils, neutrophils and reticulocytes.
For most cancer patients, undergoing tests is a serious burden, so after the study they are recommended to rest in bed.
Tumor markers for colon and rectal cancer: names, how to take tests, norm, explanation
The search for new methods of preventive diagnosis of cancer is an important area of modern medicine. After all, detecting a cancer tumor at an early stage is the key to its successful treatment.
Modern diagnostic laboratories offer a variety of panels of tests to identify markers of cancer processes using blood tests.
Let's try to figure out what tumor markers are and in what cases it is necessary to take tests to determine their number.
What are tumor markers?
A tumor biomarker is a substance (usually a protein molecule) produced either by the cancer cells themselves or by other cells of the body in response to cancer pathology.
Sometimes healthy cells in the body are able to produce such substances in response to certain benign (non-cancerous) conditions.
Tumor markers provide information about a tumor, such as how aggressive it is, whether it can be treated with targeted therapy, and how well the tumor responds to treatment.
Tumor markers are proteins or other substances that are produced by cancer cells in higher quantities than normal cells. These biomarkers are found in blood, urine, stool, or other body tissues or fluids.
For some types of neoplasia, the level of a tumor marker reflects the stage (extent) of the disease and/or the patient's prognosis (the likely outcome or course of the disease). An example of this type of tumor marker is α-fetoprotein, which is measured in the blood to assess the stage, prognosis, and track response to treatment of germ cell tumors.
However, increasingly, genomic indicators such as mutated forms of genes, tumor gene expression patterns, or nongenetic changes in the DNA of cancer cells are being used as tumor markers.
Currently, about 60 tumor markers have been characterized in detail and are in clinical use. Some of them are associated with only one type of tumor (specific tumor markers), while others are associated with several types of cancer pathology (nonspecific tumor markers).
This number does not include tumor markers, which are tested using immunophenotyping and immunohistochemistry, which help diagnose cancer and distinguish between tumor types.
At the same time, a “universal” tumor marker that could detect the presence of any type of cancer pathology has not yet been discovered.
Is preparation necessary?
Analysis for cancer cells in the body does not require special measures, but certain rules must be followed to minimize deviations of the results from the true ones. Tumor growth markers are very sensitive to external and internal environmental factors, so this cannot be ignored. Preparation for donating blood includes the following:
Taking tests requires preliminary preparation, which includes proper nutrition and limiting food intake ten hours before the procedure.
- 3-4 days before the study, the patient must adhere to dietary recommendations: exclude junk food, fried, smoked, salty foods, easily digestible carbohydrates, alcohol.
- The last meal should be at least 10 hours before the test.
- Donate blood for tumor markers on an empty stomach. You are allowed to drink mineral water without gas.
- To properly prepare for the examination, you need to refrain from smoking for a day before the diagnostic procedure.
- It is necessary to discontinue all medications that affect hormonal levels or the activity of organs that are suspected of oncology. If this is not possible or will significantly affect the patient’s condition, it is necessary to inform the doctor exactly what medications the patient is taking.
- It is recommended to cancel all physiotherapeutic procedures 2-3 days before donating blood.
What are tumor markers?
There are two main types of tumor markers that are used in different ways in oncology—circulating tumor markers and tumor tissue markers.
Circulating tumor markers may be found in the blood, urine, stool, or other body fluids of some patients. Circulating tumor markers are used to:
- forecast assessments;
- detection of tumor that remains after treatment (residual disease) or recurrence;
- assessing response to treatment;
- control the development of tumor resistance to treatment.
Although elevated levels of a circulating tumor marker may indicate the presence of a tumor, this alone is not sufficient for diagnosis. For example, non-cancerous diseases can sometimes cause elevated levels of certain tumor markers. Additionally, not everyone with a certain type of cancer will have higher levels of a tumor marker associated with that cancer.
Therefore, measurements of circulating tumor markers are always combined with the results of other tests, such as biopsy or imaging, to diagnose cancer.
Tumor markers may also be measured periodically during cancer treatment. For example, a decrease in the level of a circulating tumor marker may indicate that the tumor is responding to treatment, whereas an increase or unchanged level may indicate that the tumor is not responding.
Circulating tumor markers can also be measured after treatment ends to check for recurrence.
Examples of circulating tumor markers
- Calcitonin (measured in the blood), which is used to assess response to treatment, screen for recurrence, and assess prognosis in medullary thyroid cancer.
- CA-125 (measured in the blood) to monitor how well treatment is working for ovarian cancer.
- Beta-2 microglobulin (measured in blood, urine, or cerebrospinal fluid) to assess prognosis and monitor response to treatment for multiple myeloma, chronic lymphocytic leukemia, and some lymphomas.
Source: https://gpk1.ru/zabolevaniya/obshchij-onkomarker-na-onkologiyu.html
Analysis
For analysis, blood is taken from a vein, and stool analysis is also possible. The analysis is carried out in a laboratory equipped for immunological studies. Mostly they are located at oncology centers. Private laboratories also determine cancer markers, but some tests may not be performed there. In order not to waste time, it is better to first find out what tumor markers are determined there.
We recommend reading: Children's psoriasis. Treatment of psoriasis in children. Only lazy mothers have sick children!
Before the study you need to prepare:
- 5 days before the study, the doctor stops taking cytostatics and other drugs that affect the results. If he said that medications must be taken, then this factor will be taken into account when deciphering the results.
- Do not drink alcohol, give up cigarettes (at least for 3 days). Alcohol and nicotine significantly increase the concentration of some tumor markers in the blood.
- The day before the analysis, exclude physical activity.
- Blood from a vein is donated on an empty stomach. You cannot eat for 12 hours, and drink tea, coffee, or other drinks for 6 hours before blood sampling.
- Before donating blood for analysis, you need to sit in front of the office for 10–15 minutes to calm down.
Before submitting stool for determination of Tu M2-RK, you must not:
- undergo X-ray and endoscopic examination;
- use laxatives;
- give enemas.
Feces are collected in a sterile container.
To correctly diagnose and evaluate the effectiveness of treatment, it is not enough just to detect the presence of tumor markers in the blood. The data obtained must be interpreted correctly.
Nonspecific
Nonspecific tumor markers of intestinal cancer include those substances whose concentration rarely increases in this disease, and those that increase in any type of tumor:
- SA-125. This marker is specific for screening for ovarian cancer, but its concentration is significantly increased in tumors of the gastrointestinal tract.
- SA-242. The determination of this tumor marker is used to identify tumors of all organs of the gastrointestinal tract. It has the highest specificity (95%) for diagnosing pancreatic cancer.
- SCC. This is an antigen for squamous cell carcinomas. Detected in the blood for squamous cell cancer of the anus, vulva, esophagus, cervix, etc.
- AFP (alpha fetoprotein). It is used to detect primary liver cancer. A significant increase in tumor marker is observed with metastatic liver disease.
- CYFRA 21-1. The cytokeratin fragment is a marker of epithelial tumors. Its concentration in rare cases increases with intestinal cancer.
- Trophoblastic Pj-globulin. A significant increase is observed with chorionic carcinoma, chorionepithelioma, and extremely rarely with intestinal cancer.
- TRA. Cytokeratin. Its amount increases significantly with malignant changes in the epithelium. Indicates cancer of the colon and rectum, breast, lungs, cervix, bladder and inflammatory diseases.
- TPS. It is an epitope of cytokeratin. Determination of its concentration is used to monitor the effectiveness of treatment of patients with stomach, breast, prostate, and colorectal cancer.
A referral for tumor marker testing is given by an oncologist . It is the doctor who determines which of the specific and nonspecific indicators of malignant formations are important for diagnosing intestinal cancer and differentiating the disease from benign diseases.
The main thing about colon cancer
According to modern data, colon cancer in its various parts is the leading oncological disease of all organs of the gastrointestinal tract. It surpasses even stomach cancer in frequency. This disease is most common in civilized countries, such as Western Europe and North America. In those countries where people engage in physical labor and do not have bad habits, for example, among the poor population of Asia and Africa, the incidence of colon tumors is very low. In our country, about 30 people out of every hundred thousand fall ill every year, or 1 person out of 3,000 randomly selected.
At the same time, early appeal and, accordingly, early detection are extremely low, if we talk about Russia. More than 60% of all newly diagnosed cases of malignant neoplasms of the large intestine are already advanced cases of the third and fourth stages, with the presence of distant metastases, tumor disintegration and bleeding. At such a late stage, even a general blood test for colon cancer can be diagnostically important, but people stubbornly cling to false thoughts about hemorrhoids and are simply afraid to go to the oncologist.
It should be remembered that the risk factors leading to carcinogenesis are the following:
- A small amount of plant foods and fiber in the diet: colon cancer very rarely develops in people with a normal bowel movement rhythm who regularly eat fiber, bran and various dietary fibers;
- The desire to consume as many animal products as possible, especially those that have undergone long-term processing. These are sausages, canned food, smoked meats, spicy foods and spices;
- A significant risk factor is a sedentary lifestyle, which leads to constipation;
- The presence of chronic intestinal dysbiosis.
According to pathological studies, more than half of all tumors are rectal tumors. Then gradually the likelihood of tumors decreasing. The sigmoid colon accounts for 20%, the descending colon - 15%. Transversely, the colon is affected in about 7% of cases. And the initial section of the large intestine, or ascending colon, serves as the site of tumor formation in only 6% of cases.
Almost all malignant neoplasms of the large intestine, according to histological characteristics, belong to adenocarcinomas, which resemble polyps, bleeding ulcers, or mucosal defects similar to craters with dense edges.
What to do if tumor markers are detected?
An increased concentration of tumor markers is in no way a criterion for diagnosing cancer. These substances may appear in greater quantities in the blood during benign diseases. In addition, determining the concentration of tumor markers over time has the greatest diagnostic value: has their number decreased or increased after surgery or conservative therapy. Such screening studies are carried out monthly, if metastases are suspected, to monitor the growth of a tumor that cannot be removed for one reason or another.
To diagnose intestinal cancer, especially in the early stages, analysis of tumor markers is not enough. If only because these substances enter the bloodstream during intensive tumor growth.
A doctor will suspect bowel cancer when a patient comes to him with the following alarming symptoms:
To identify malignant intestinal tumors, the following is carried out:
- digital examination of the rectum;
- sigmoidoscopy;
- irrigoscopy;
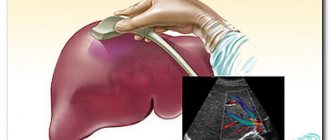
- MRI, CT, ultrasound;
- radionuclide studies;
- endoscopy with biopsy.
The most accurate data is obtained by performing a biopsy and subsequent study of tissues and cells - histological examination. It allows you to determine the stage of cancer and therapeutic strategy.
Tumor markers are substances that are produced by tumor cells or nearby cells. To diagnose and monitor the effectiveness of treatment of malignant intestinal tumors, an immunological study is performed to identify tumor markers. Their concentration is influenced by the aggressiveness of tumor growth and the extent of the process, which makes it possible to suspect cancer and evaluate the effectiveness of therapy, and determine the degree of radical intervention.

When interpreting the obtained data, not only the concentration of tumor markers is taken into account, but also their specificity and sensitivity. Some indicators are also influenced by other factors. CEA is increased in smokers and alcoholics.
Among cancer diseases, intestinal cancer is of significant importance. Intestinal tumor markers are used to promptly identify symptoms characteristic of a given situation. Thus, the development of the pathogenic process is determined. You should understand the mechanism of operation of these substances and find out what laboratory tests are necessary.
When and how are tests taken?
All tests for stomach tumor markers are taken in the morning, on an empty stomach. There are also dietary restrictions the day before the test.
What are the requirements for the obtained result to be as reliable as possible?
- Do not eat 12 hours before the test.
- If you are taking the vitamin biotin, you must stop taking it 8 hours in advance.
- 48 hours before donating blood, do not eat anything fried, fatty or spicy. Only boiled, steamed food that does not cause irritation to the mucous membranes.
- You should also not smoke, drink coffee, tea or even mineral water. It is permissible to drink only clean water.
Smoking patients are warned that cigarettes are also prohibited several hours before the procedure. Smoking may also affect the results. By the way, tobacco smoke contributes to the development of stomach cancer. Since carcinogens enter the organ directly with it. And besides, nicotine enhances the production of hydrochloric acid.
Features of indicators
So, the following tumor markers of the small intestine are distinguished:
- a type characterized by the development of a progressive type of cancer. This type is called highly specific;
- a type that helps confirm the presence of a malignant tumor. This is a non-specific type of marker.
Malignant neoplasms can reveal:
- CEA markers are particularly sensitive. The tumor marker of the large intestine is in the normal range – up to 5 units. Its absence is also possible;
- antigen CA72 – 4 is responsible for effective diagnosis in the field of colorectal oncology. A value of up to 6.3 is considered a normal level;
- indicates metabolic processes in the area of pathogenic Ti M2 cells - RK;
- If the CA19-9 value is exceeded, conclusions can be drawn about the presence of cancer. The norm fluctuates around 40 units;
- at the stage of initial development of cancer, CA 242 is detected. The optimal level is considered to be 0 – 30 units.
It is also worth noting that exceeding the normal level of the indicator is not a 100% guarantee that an oncological process is present. When observing this situation, it is necessary to conduct additional examination, in particular basic tests.
We recommend reading: Allergy to mascara: symptoms and what to do
Gastrointestinal tumor marker 72-4
Let's take a closer look at each of the markers. What tumor markers are tested for stomach cancer? So, Tumor-associated glycoprotein 72-4 is a marker for carcinoma. This could be a tumor of the stomach, pancreas or lungs. A persistent increase in the blood of these glycoproteins indicates the presence of either a benign or a malignant tumor. But it is also present in the body of pregnant women. Venous blood is taken for analysis. The reference value is up to 6.9 units/ml.
Unfortunately, no marker can accurately determine the location of the tumor. The diagnosis can only be made by a council of experienced and highly professional oncologists after collecting anamnesis and having the results of all tests available.
Deciphering the tumor marker
You should learn about the characteristics of tumor markers.
A normal amount of CEA is produced during pregnancy by the body's digestive system. Based on the analysis data, it is possible to accurately determine the size of the tumor and evaluate this indicator for the further course of treatment. By assessing the marker, it is possible to predict possible relapses in the near future.
CA 19 – 9 is considered additional, which is assessed after the above markers. Among his main functional responsibilities is the ability to diagnose possible relapses. The marker is also able to detect the presence of a tumor in the ovarian area. With the help of its monitoring, qualified specialists monitor the effectiveness of treatment and its effect on the gastrointestinal tract.
The next, rather specific protein, CA 242, is generated in the rectum area, as well as in the large intestine. Thanks to its assessment, it is possible to determine the presence of a tumor of a certain period. This value is in the range from 3 months to 6.
There are also other types of tumor markers. In particular, this is CA 125, it is used to diagnose the sigmoid colon. This group includes SYFRA 21 - 1, which indicates the presence of a cancerous tumor in the rectal area. SCC determines the oncological process in the rectal canal area.
First screening. What tests are taken?
Screenings are carried out to determine risk groups. These types of tests are not diagnostic. However, they are necessary to understand whether further research is needed and whether a person should spend money and time on other tests, analyzes and complex studies.

Primary tumor markers are proteins whose enzymes are waste products of the tumor. They are determined first, as they have greater sensitivity. They use CA 15-3, CEA, CA-50 and an additional analysis - a marker for pancreatic carcinoma CA 242. The gastric tumor marker CA 72-4 is most informative for making a diagnosis.
Intestinal oncology
It is worth understanding the structural features of the intestines. Its main components are the small and large intestines. The small intestine includes the duodenum, ileum, and jejunum. Considering the structure of the large intestine, it is worth noting the cecum, rectum and colon, which are its constituent components. The rectum area ends at the anus. Pathological processes of development of neoplasms are observed in different places. A person feels constipated, which is natural if there is a tumor. It helps block the movement of bowel movements along its natural path.
There are several effective ways to determine the disease at the initial stage of development. This diagnosis includes a tumor marker for colon cancer.
They represent a special kind of chemical substances, in other words proteins, which can be identified using biomaterials. The components can be produced both by malignant cells and neighboring organs. During diagnosis, the protein indicator, subject to the development of cancer, is at an exceeded level. Urine, blood, and in fairly rare cases, feces are used for analysis and evaluation of results.
Important! Tumor markers perform functional work, which is manifested in effective treatment monitoring. Their use helps determine the effectiveness of the course prescribed by a specialist.
Important! Tumor markers perform functional work, which is manifested in effective treatment monitoring. Their use helps determine the effectiveness of the course prescribed by a specialist.
Normal indicators
In people without pathology, blood tests for cancer markers correspond to the following values:
- CEA is defined as 0-3 ng/ml.
- Normally, CA 72-4 is not present in the blood, but an increase in the test result to 4 units in 1 ml of blood is allowed.
- SCC in the absence of pathology is 0-2.5 ng in 1 milliliter of the test material.
- CA 19-9 and CA 125 cannot be more than 37 U/ml.
- AFP in the absence of cancer does not exceed 15 ng/ml.
- Up to 20 units, CA 242 and LASA-P indicators are not pathological.
- Tu M2-RK cannot exceed 15 units.
- CYFRA 21-1 is normally absent in the body.
An increase in cancer markers in people without the disorder is called a false positive. This can happen if there are inflammatory processes in the organs of the digestive tract, organic changes, or benign formations. An incorrect result is also possible due to violation of the rules for preparing for analysis. Therefore, it is necessary to take a comprehensive approach to interpreting the level of tumor markers in order to prevent diagnostic errors.
Tumor markers for colon cancer
Tumor markers can be divided into groups, and if they are determined together, the likelihood of detecting a malignant neoplasm increases. Thus, in modern laboratory diagnostics there are also tumor markers for intestinal cancer - these are CEA and the tumor marker CA 19-9. If you study them together, you can assess the prognosis of the disease, as well as monitor treatment. And we are talking, first of all, about colon cancer.
Carcinoembryonic antigen (CEA)
A separate page is already dedicated to this tumor marker on our website REA tumor marker: indicators, norm, interpretation of the analysis, but now we will consider it as one of the tumor markers for intestinal cancer.
This is a combination of protein and carbohydrate, and in its physical structure the antigen molecule is similar to immunoglobulin, or antibody molecules that protect our body. Normally, the concentration of this substance in a healthy person may even be different from zero, since this substance is synthesized in the large intestine, and sometimes its amount reaches detectable values. Its function has not been fully elucidated; it is believed that the embryonic antigen carries out subtle interactions between cells and takes part in indirect reactions of local immunity.
However, oncologists are well aware that there is a direct connection between increased CEA concentrations and cancer activity. It grows when it enlarges, grows into the deep layers of the intestine (or invasive growth), and also when it metastasizes. It is noted that the later a malignant neoplasm is detected, the larger the tumor, the higher the level of CEA in the blood plasma the patient will have.
Early, subclinical stages of tumor development do not lead to a significant increase in CEA concentration. Unfortunately, this analysis will not always be valid in the case of large tumors at later stages. In approximately 15% of all patients with newly diagnosed late-stage colon cancer, CEA was normal.
The specificity of this analysis alone is also low. It can also increase in the presence of other diseases that are not related to malignant neoplasms. This could be hepatitis, chronic colitis, pancreatitis. High CEA can occur in patients with long-term obstructive processes in the lungs, and in women various forms of endometriosis cause an increase in its concentration. In addition, high concentrations of CEA can be observed in cancer tumors of extraintestinal etiology. These are ovary, kidney and breast tumors.
However, if the diagnosis of intestinal cancer has already been made and confirmed histologically, then the diagnostic value of the carcinoembryonic antigen increases against the background of the existing tumor. If surgical removal is necessary, this analysis must be performed again. It is better to operate against the background of low CEA values, or even if they are high, but there is still a tendency for them to decrease. According to statistics, such surgical intervention will have a greater chance of success. If the patient again experiences an increase in CEA concentration after surgery, then most often the tumor has recurred.
Tumor marker CA 19-9 (carbohydrate antigen)
The second intestinal tumor marker, which is taken together with CEA, is carbohydrate antigen, or CA 19-9. This is also a complex protein combined with a carbohydrate, and, as in the first case, a separate analysis is not highly sensitive and highly specific. You can get acquainted with it in more detail on the page What does a blood test for the tumor marker CA 19-9 mean?
It can also occur with pancreatitis, with liver diseases, not only with colorectal cancer. It does not determine the type of tumor: it does not matter what kind of cancer the patient has. The concentration of intestinal tumor markers, and in particular CA 19-9, does not depend on its histological structure.
A feature of the intestinal carbohydrate tumor marker can be considered its lower sensitivity than that of CEA. Each of these tumor markers has its own specific characteristics of sensitivity and specificity, so their joint determination is necessary. As a result, both sensitivity and specificity are increased. In modern clinics, when it comes to laboratory diagnosis of colon cancer, only these two tumor markers are used together. It makes no sense to use them separately, since in this case the risk of errors will be higher.
In addition, even if intestinal tumor markers are positive, and this concerns two antigens at once, there is no 100% basis for making a diagnosis of a malignant neoplasm. The result of a blood test for intestinal cancer must be confirmed by determining tumor markers. Confirmatory tests will be the results of instrumental studies, but first of all - a biopsy with histological analysis and determination of the morphological, cellular type of the neoplasm.
Carrying out analyzes
To study tumor markers, venous blood is needed. For the convenience of patients, it is recommended to carry out the procedure in a lying position. The material is handed over in the morning. The duration of the diagnostic procedure is no more than 15 minutes. The resulting material is placed in a sterile container and sent for examination. Each marker requires specific reagents and implementation features. Therefore, the result is provided within 6-7 days.
The tumor marker for intestinal cancer Tu M2-RK is different from others. To conduct the study, the patient's stool is needed. Before this, you should not use laxatives or an enema to make the analysis more informative. Several particles are isolated from different sections of the material and the concentration of Tu M2-RK, a special substance that characterizes the metabolic processes of the tumor, is determined.
To diagnose a malignant process using tumor markers, special care is needed. The permissible error in the laboratory is 15-20%.
Types of tumor markers
In the early stages, the development of a tumor in the intestine is extremely difficult to determine. You need to pay attention to the appearance of symptoms such as frequent constipation and bloating. These are the first signals to see a doctor and undergo testing for intestinal tumor markers. In clinical practice, about 20 tumor markers are used to identify tumors in the human body. Among them, there are two types of pathological proteins:
- nonspecific. They confirm the presence of a tumor in the body, but do not determine the specific location of its formation;
- specific. Such tumor markers reveal not only a cancerous tumor, but also its location in the human body.
What tests are there?
A general blood test for intestinal cancer is not informative. It is able to detect increased ESR in oncology and anemia, but this is not specific for detecting carcinoma. For this reason, other substances that are synthesized during malignant neoplasms are detected in the blood. Intestinal tumor markers are divided into 2 large groups:
An examination for intestinal tumor markers is a study of blood for substances produced in tumor diseases of the digestive tract. This is a laboratory method for confirming or refuting a diagnosis, which is used before complex and unsafe instrumental research methods. Diagnosis does not take much time and does not cause significant discomfort.

An increase in cancer markers in people without the disorder is called a false positive. This can happen if there are inflammatory processes in the organs of the digestive tract, organic changes, or benign formations. An incorrect result is also possible due to violation of the rules for preparing for analysis. Therefore, it is necessary to take a comprehensive approach to interpreting the level of tumor markers in order to prevent diagnostic errors.
Let's work together to make the unique material even better, and after reading it, we ask you to repost it on a social network convenient for you. net.
Indications for donating blood for tumor markers
For what purposes are marker tests taken? What can tumor markers indicate?
- Blood is given for analysis for the purpose of primary diagnosis.
- If the diagnosis is already clear, then to make a treatment prognosis.
- To evaluate the performance of treatment already performed. After a course of chemotherapy, tumor markers must be taken again.
- In order to detect metastases in the body several years after successful treatment.
Who needs to take primary blood tests for stomach tumor markers? Tests are primarily given to people at high risk of cancer. These are people who already have the following diseases:
- severe atrophic gastritis;
- peptic ulcer;
- adenomatous polyps in the stomach.
The risk is increased in former surgery patients who have had part of their stomach removed.
Oncologists know how quickly the Correa cascade progresses. Over the course of 10-15 years, cancer develops from atrophic gastritis along the following chain of diseases - atrophy - metaplasia - dysplasia - cancer.
The risk is also high if there are close relatives suffering from any type of tumor, and who work in unfavorable conditions (increased levels of radiation).
Where to get tested for intestinal tumor markers
We offer to undergo such an examination at our City Medical Center. Modern equipment, qualified staff and reasonable prices for our services are the advantages thanks to which patients return to the clinic when necessary. The analysis results will be ready within one day. They are sent by email, which saves the patient’s time because there is no need to come to the clinic for the results. If you do not have the opportunity to visit our laboratory, you can call a nurse to your home and receive the final results by email.