Sections of the colon
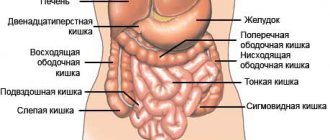
Features of the anatomical location of the intestine in the abdominal cavity made it possible to divide it into 4 sections:
- Ascending colon.
- Transverse colon.
- Descending colon.
- Sigmoid colon.
The total length of the four parts reaches 1.5 -2 meters.
Ascending colon
The intestine is located to the right of the midline of the abdomen (right flank) in the abdominal cavity. Being a continuation of the cecum, it rises up to the lower edge of the liver. At this level, it forms the right flexure of the colon (hepatic flexure) and passes into the transverse part of the large intestine. The length of the ascending part is about 15-20 cm. The ascending part is topographically limited from behind by the quadratus dorsi muscle and the right kidney, above by the right lobe of the liver and gall bladder, in front by the anterior abdominal wall, and inwardly by loops of the small intestine. In a small number of people, the intestine has its own mesentery, which ensures its mobility and the development of volvulus of the cecum and colon (in rare cases).
Transverse colon
The ascending and descending sections of the large intestine are connected to each other by the transverse colon. The intestine is located in a horizontal plane, slightly sagging downwards. It originates from the hepatic flexure and reaches the left hypochondrium, forming the splenic flexure (left flexure of the colon). The left flexure is located above the right flexure of the colon. When palpating the abdomen, it can be detected above the navel in the form of a horizontal elastic cord.
The length of the transverse colon varies from 25 cm to 65 cm in an adult. The transverse colon is bounded on the right by the liver, on the left by the stomach and spleen. The duodenum and pancreas are located behind the intestine, and the loops of the small intestine are adjacent below. The anterior part is covered by the anterior abdominal wall. In the abdominal cavity, it is attached to the walls using the mesentery.
Descending colon
It starts from the left flexure of the colon and descends to the left iliac fossa, passing into the sigmoid colon. Posterior to the intestine lies the left kidney and the quadratus dorsi muscle. Covered in front and left by the abdominal wall. The right side of the descending colon is adjacent to the loops of the small intestine. The length of an adult varies from 10 to 30 cm.
We recommend reading:
More about hemorrhoids: causes, symptoms and treatment methods
Sigmoid colon
It is located in the left iliac region and forms 2 loops: proximal and distal, which lie on different muscles. The proximal part is supported by the iliacus muscle, and the distal part by the psoas major muscle. The length of the sigmoid colon can be from 15 cm to 50 cm in an adult. Near the intestine there is the left ovary, uterus, and bladder.

Waste
The amount of feces produced during the day varies from almost 500 g (if the food is rich in vegetables and fruits) to 200 g (if animal proteins predominate in the food) and 30 g during fasting. Although active absorption occurs during the digestion process, stool typically contains 65-80% water. Half of the remaining dry matter is bacteria (mostly non-living), and the rest is colonic secretions, cellular debris from the gastrointestinal tract, and small amounts of undigested food. Fiber predominates in leftover food (hence the abundance of feces on a vegetarian diet). The color of stool depends on bile dyes. The strongest smell comes from a meat diet, a weaker one from a vegetable diet, and the least strong from a dairy diet.
Wall structure
Located in the abdominal cavity, throughout the entire length of the wall of the colon are formed by the following layers (membranes):
- slimy;
- submucosal;
- muscular;
- serous.
The mucous membrane lines the inner surface of the intestine. It contains epithelial cells, between which there are a large number of endocrine glands. The glands bend to form crypts. Each crypt contains goblet cells that produce mucus to facilitate the passage of feces. The surface of the crypts is dotted with cells with a set of villi and enzymes for breaking down substances that enter the intestines. The mucous layer also contains blood vessels, clusters of lymphatic plaques (follicles), nerve endings and single muscle fibers. Lymphatic follicles are of great importance in the development of immunity in childhood. Protrusions of the mucous wall increase the absorption surface of the intestine several times.
The submucosa is a connective tissue with a high content of nerve fibers, lymphatic follicles, and blood vessels.
The muscular coat is formed by thick layers of internal muscle fibers (circular layer) and external fibers (longitudinal layer). Nerve plexuses are located between the layers. The longitudinal layer consists of three ribbon strands throughout the entire colon. Between the muscle fibers, the intestinal walls protrude, forming haustra. The haustrae are separated by circular muscle fibers. Contraction of haustra ensures better movement of feces.
The serosa is the outer lining of the colon. There are fatty growths on its surface. The role of the processes is not fully understood.
Functions
- Absorption of water and salts. Every day, up to 2 kg of food mass (chyme), which is largely represented by water, enters the large intestine. The intestines absorb from 1.4 to 1.9 liters of water per day, mainly in the ascending colon. Salts of sodium, potassium, chlorine, and calcium are also absorbed in the colon. After absorption of all the necessary electrolytes and water, 200-300 g of intestinal contents remain, which is formed into feces.
- Formation of feces. With the help of peristaltic movements, the intestinal contents are mixed and gradually moved towards the rectum. The descending colon and sigmoid colon accumulate feces, which, at a certain mass, create pressure on the sphincter in the rectum and cause the urge to defecate. This accumulation allows you to avoid the constant release of feces from the intestines in an unregulated manner.
- Synthesis of vitamins (group B and vitamin K). The main source of B vitamins and vitamin K are intestinal bacteria.
- Mucus formation. The secretion of mucus by goblet cells in the large intestine allows stool to move better through the intestines. There are practically no enzymes in mucus.
- Digestion. Compared to the small intestine, the colon is practically not involved in digestion. Absorption of small amounts of glucose and some amino acids synthesized by intestinal microorganisms may occur.
Read on: Where does the digestion process begin?
Diseases of the small intestine
The most common ailments that affect parts of the small intestine are diarrhea and fecal retention in the tract. Defecation disorders are often accompanied by the development of pain syndromes in the peritoneal area. Quite often, with poisoning and disorders of the small intestine, excessive gas formation is observed. In this case, the pain is short-lived, moderate in nature and is not the main factor of discomfort.

A common symptom of the development of malfunctions in the small intestine is rumbling in the peritoneum, a feeling of atypical movement in the abdomen. Most often, such manifestations are a consequence of abundant gas formation as a result of consumption of legumes, cabbage, potatoes, and rye bread. These symptoms may intensify significantly at night.
Failures in the production of enzymes and the breakdown of food gruel into microelements lead to more serious consequences. If food absorption, due to the absorption of substances into the blood and lymphatic vessels, does not occur properly, this can lead to weight loss and weakening of bone and muscle tissue. The consequences of digestive disorders are often hair loss, dry skin, and swelling in the extremities.
There are several main conditions that lead to the development of pathologies in the small intestine:
- Malabsorption is a malabsorption of nutrients.
- Maldigestion is low digestive activity.
If we talk about insufficiently high-quality processing of food gruel, such phenomena arise against the background of a low content of enzymes in intestinal juices. Low fermentation can be either acquired or genetic. Typically, pathologies of this type are a consequence of chronic inflammation, endocrine diseases, and surgical interventions.

Methods for diagnosing the colon
- X-ray of the abdominal organs with contrast. It is the main method for diagnosing diseases of the colon. The method is based on the penetration of X-rays through the intestine, which contains a radiopaque substance (barium suspension), and obtaining images. Using this method, developmental anomalies and intestinal obstruction can be diagnosed. Assess the condition of the intestinal mucosa, tone and peristaltic movements, the speed and nature of the movement of barium suspension through the intestine. The disadvantages include the difficulty of diagnosing tumors in the early stages of development.
- Colonoscopy. An endoscopic diagnostic method, which is based on visual examination of the inner wall of the intestine using an endoscope. Under visual control, the doctor can judge the condition of the mucous wall, identify organic pathology (polyps, erosions, tumors), and take biopsy material. The disadvantages of the study include the presence of a special preparatory stage before the study, the painfulness of the procedure, and the inability to evaluate other intestinal linings.
- Computed tomography (CT). A modern diagnostic method is based on the penetration of X-rays into the abdominal cavity in different planes simultaneously and reading information by several sensors at once. Using a computer program, an image of the intestines and surrounding organs and tissues is obtained in several planes. CT reveals tumors with minimal size, metastases, organic pathology, inflammatory changes, and developmental abnormalities.
- MRI (magnetic resonance imaging). The method is based on layer-by-layer examination of the required area of the body using magnetic fields. MRI is used to diagnose neoplasms, inflammatory processes in the intestines, and metastases in surrounding tissues. It is a safe research method. Not used only if there are metal objects in the body.
- Ultrasound. Advanced ultrasound diagnostics allows you to examine the intestines. Ultrasound reveals tumors in the intestinal wall, inflammatory changes in the walls of the colon. At the same time, nearby organs and tissues can be examined.
- Endoscopic ultrasound diagnostics. A type of ultrasound diagnostics is this method, which is based on the introduction of an ultrasound sensor into the intestinal lumen through the rectum. This position of the sensor allows you to accurately determine from which intestinal lining the tumor is growing, and to determine the presence of compression of surrounding tissues.
- Diagnostic laparoscopy. An invasive method that is based on microsurgical insertion of endoscopes through incisions in the anterior abdominal wall. More often it combines diagnostic testing and surgical treatment (removal of part of the intestine).
We recommend reading:
Cryptitis: definition of pathology, symptoms and treatment methods
In continuation of the topic, be sure to read:
- Sigmoid colon: location, structure, functions and diseases of the organ
- Diseases of the sigmoid colon: symptoms and signs of disease, their treatment
- Sigmoiditis (inflammation of the sigmoid colon): symptoms and treatment methods
- Proctitis: symptoms and treatment methods (diet, drugs, surgery)
- Preparation and performance of intestinal sigmoidoscopy
- Intestinal dolichocolon in adults: definition of pathology and treatment
- Details about the intestines: structure, sections and functions of the organ
- Large intestine: location, structure and functions
- Diseases of the colon: symptoms and signs of pathologies, treatment
- Intestinal colonoptosis: definition, symptoms, treatment and prognosis
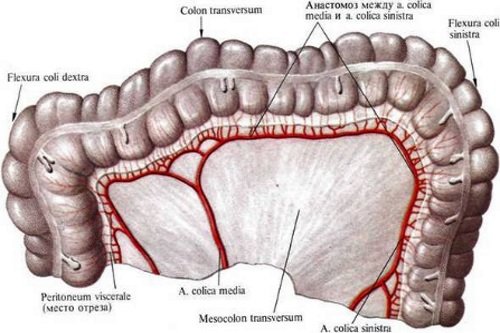
Blood supply and innervation
The blood supply to the organ is provided by two main vessels that arise from the abdominal aorta. These are the superior and inferior mesenteric arteries.
Innervation is provided by the branches of the superior and inferior mesenteric plexuses and the branches of the celiac plexus.
The nerve branches of the superior plexus innervate the appendix, cecum, ascending and transverse colon.
Closer to the intestinal walls, the branches divide into smaller branches.
Innervation of the rectum is provided by branches coming from the sacral section of the sympathetic trunk.