In most cases, this is a complication after myocardial infarction, atrial fibrillation or slow sepsis. The disease occurs due to embolism and thrombosis of the mesenteric vessels.
The pathology affects elderly and middle-aged people, since atherosclerotic changes occur in the vessels throughout life.
A thrombus blocks the lumen of arteries or veins, which disrupts the nutrition of the intestinal walls, leading to infarction of the affected tissues.
Venous thrombosis is observed much less frequently than arterial thrombosis. In rare cases, blockage of veins and arteries is diagnosed at the same time; this form is called mixed.
Why is blood flow disrupted?
The lumen of the vessels can be blocked primarily or secondary. In the first case, the causes are injuries, thrombosis and embolism, and in the second, the disease develops as a result of prolonged changes in the walls of blood vessels or outside them.
Primary reasons include:
- Injuries – strong blows to the abdominal area;
- Myocardial infarction;
- Cardiac aneurysm and other pathologies of the cardiovascular system.
Pathological factors can be different (embolism, trauma or thrombosis), but they all lead to intestinal ischemia.
The following are considered secondary reasons:
- Stenosis of atherosclerotic origin;
- A decrease in cardiac activity, in parallel, a drop in blood pressure occurs;
- Tumors of the small or large intestine that compress the arteries;
- Surgeries on the aorta performed to reconstruct the vessel.
Thrombosis of intestinal vessels
- Causes of thrombosis
- Main features
- Treatment of the disease
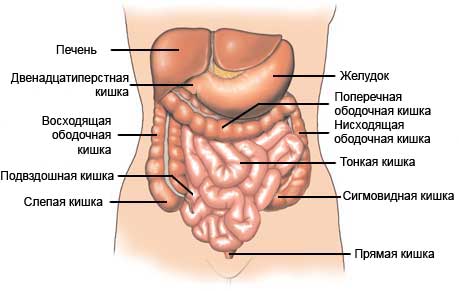
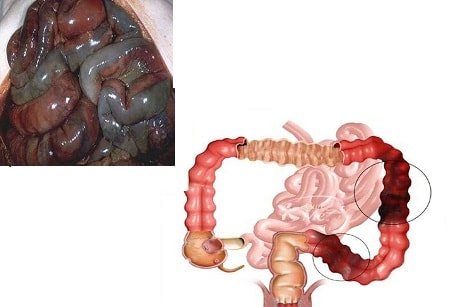
The human intestine is supported by a special tissue - the mesentery, the vessels of which supply the organ with blood.
Each of these vessels (they are called mesenteric) is responsible for supplying blood to a specific area of the intestine. When blood circulation is impaired in the vessels of the mesentery, mesenteric thrombosis develops. In essence, this acute condition is an intestinal infarction and often ends in death.
While myocardial infarction is easily diagnosed, intestinal thrombosis is difficult to detect, especially at the onset of the disease.
This pathology occurs mainly in middle-aged and older people, regardless of gender. Intestinal infarction most often develops with acute occlusion of the trunk or mouth of the superior mesenteric artery. The trunk is usually divided into three segments; in case of thrombosis or embolism of each of them, a certain localization of intestinal damage is observed.
When the first segment is blocked, most patients experience thrombosis of the small intestine, as well as the blind and right half of the colon.
With occlusion of the second segment, the entire ileum and part of the jejunum, rarely the ascending colon and cecum, are affected.
When the third segment is blocked, the blood circulation is usually compensated, and during a heart attack only the ileum is affected.
Causes of thrombosis
Intestinal thrombosis occurs as a result of atherosclerosis of the mesenteric vessels. A plaque forms in the artery, which narrows the lumen and impedes blood flow. In the worst case, the vessel is completely blocked, and as a result, the blood supply to any part of the intestine is disrupted.
The affected area does not receive normal nutrition, as a result, destructive changes occur in the intestinal wall. This process begins from the mucous membrane with the appearance of ulcers and necrosis. Then the tissue disintegrates and the intestine perforates, that is, a hole is formed in it through which the contents of the intestine enter the abdominal cavity.
In this case, peritonitis develops, which can lead to death.
The causes of intestinal thrombosis may be the following:
- atherosclerosis;
- hypertonic disease;
- heart defects;
- heart attack;
- cardiosclerosis;
- obliterating endarteritis;
- liver and spleen diseases;
- abdominal trauma;
- malignant tumors;
- complications after surgical operations on the abdominal organs.
Main features
Most often, arterial thrombosis begins acutely. The prodromal period (the initial stage without obvious clinical symptoms) is characteristic exclusively of arterial thrombosis. In this case, for about 1-2 months the patient complains of periodic abdominal pain, bloating, vomiting, nausea, pain after eating, and unstable stool. The cause of these symptoms is vasoconstriction due to thrombosis or atherosclerosis.
Venous thrombosis develops over several days (two to five). At the onset of the disease, there is a slight increase in temperature and unexpressed abdominal pain of uncertain localization.
Intestinal ischemia
The main symptom of intestinal thrombosis is severe pain. They are especially unbearable in the initial stage of the disease - ischemic, which lasts from 6 to 12 hours. Patients, as a rule, cannot find a place, scream, and pull their knees to their stomach. The pain is not relieved even with narcotics. Some effect can be obtained from antispasmodics.
In addition, the following symptoms are noted:
- pale and bluish skin;
- rare pulse;
- increased blood pressure.
At the same time, the stomach remains soft and the tongue moist. A blood test shows that the number of white blood cells is increased. The pain is concentrated in the epigastric region or throughout the abdomen. Symptoms such as nausea and vomiting occur; most patients experience loose stools mixed with blood; a quarter of patients experience stool retention.
We recommend reading:
Abdominal aneurysm
After 6-12 hours, the infarction stage begins. It can last up to a day. During this period, the pain subsides somewhat due to the death of pain receptors, which occurs as a result of necrosis of the intestinal wall.
Patients calm down, but due to intoxication their behavior becomes inadequate. The pulse quickens, the blood pressure returns to normal, and the number of leukocytes continues to increase.
The pain is localized in the area of the affected areas.
18-36 hours after the onset of the disease, the stage of peritonitis begins. Inflammatory processes in the abdominal cavity lead to increased pain during palpation, coughing, and body movements.
The general condition of the patients deteriorates sharply, which is due to dehydration, toxicosis, metabolic acidosis, and electrolyte imbalance. Pain is felt throughout the entire abdominal cavity.
In this condition, the patient experiences symptoms such as dry tongue, gray skin, thready rapid pulse, low blood pressure, high leukocytosis.
In the case of arterial thrombosis, if timely assistance is not provided, the course of the disease lasts two days, then death occurs due to intoxication and peritonitis. With venous, the process lasts five to six days.
Treatment of the disease
Any thrombosis of the rectum, pelvic vessels or lower extremities is fraught with serious complications. But some types, including mesenteric thrombosis, are deadly, so treatment should be started in the first hours of the disease.
If you consult a doctor in a timely manner and with a quick diagnosis, conservative treatment is possible, that is, dissolving the blood clot with special drugs that are administered intravenously. Timely therapy can restore impaired blood circulation.
Unfortunately, early diagnosis of intestinal vascular thrombosis often does not occur due to examination of other organs and exclusion of other diseases: appendicitis, acute cholecystitis, pancreatitis, and gynecological acute conditions. Therefore, surgery is often the only solution.
Before the onset of necrosis of the intestinal wall, the thrombus, part of the vessel or the entire vessel is removed, and arterial prosthetics is performed. If necrosis has begun, the following treatment is carried out: the affected area of the intestine is removed. Thus, after the operation its patency is restored.
Something to remember! Thrombosis of intestinal vessels can lead to death, and only a quick visit to a doctor, early diagnosis and timely treatment will save a life.
With this disease, the prognosis is favorable until diffuse peritonitis occurs.
Source: //icvtormet.ru/bolezni/tromboz-sosudov-kishechnika
articles
This organ is a double layer of the peritoneum, which contains not only nerve endings and lymph nodes, but also intestinal blood vessels:
- superior and inferior mesenteric arteries (blood supply);
- superior and inferior mesenteric veins (outflow of blood).
There are various painful conditions that provoke disruption of intestinal blood flow, and, accordingly, its functions. One of the most dangerous and even fatal pathologies is mesenteric intestinal thrombosis. About what kind of disease this is, what its clinical picture is, whether diagnosis is difficult and what treatment methods exist, further in our article.
Mesenteric thrombosis: causes of occurrence
As mentioned earlier, thrombosis of mesenteric vessels is a circulatory disorder that is acute in nature. The reason for its occurrence is mechanical blockage of the arterial and venous beds of the intestine.
The movement of blood through the vessels is partially or completely blocked by the formed thrombus (blood clot), which can cause irreversible consequences. Due to the lack of timely diagnosis and therapy, the disease will undoubtedly develop. Intestinal infarction is almost inevitable.
This means that part of the digestive organ will be removed, which poses a real threat to life.
Many people have probably never even heard of this disease. Therefore, it is doubly important to have at least minimal information about the disease. So what could cause it?
It is worth noting that a diagnosis such as thrombosis of mesenteric vessels is made mainly in elderly people. Because it is directly related to long-term cardiovascular diseases. Most often, in old age, people with cardiosclerosis, cardiac aneurysm and various etiologies of endocarditis develop thrombosis of the intestinal mesenteric vessels.
In addition, myocardial infarction can also cause blockage in the mesenteric vessels. After all, blood clots formed in places where the heart muscle is damaged, if they break off, can move and settle in the vessels. And after this, the clogged artery or vein is deprived of nutrition, which certainly cannot but lead to serious consequences.
Is it only in patients with atrial fibrillation and those who have suffered a myocardial infarction that thrombosis of the mesenteric arteries and veins can develop? Unfortunately, these painful conditions are not limited to the causes of the formation of blood clots and emboli in the intestinal vessels. Any disease with a risk of internal bleeding can subsequently lead to mesenteric thrombosis, namely:
- severe stages of acute intestinal bacterial infections;
- inflammation of the pancreas (pancreatitis);
- portal hypertension syndrome with an increased index of congestion inside the portal vein;
- tumors of the small or large intestine that compress the arteries;
- increased blood clotting;
- cirrhosis and steatosis of the liver.
In addition to the above diseases, arterial and venous mesenteric thrombosis can be provoked by injuries to the abdominal organs, surgery, hormonal therapy, smoking abuse and even a sedentary lifestyle.
: mesenteric thrombosis - intestinal infarction
is not responsible for the accuracy of the information presented in this video clip. Source – JitZdorovo
Mesenteric thrombosis: forms, types and stages of the disease
According to the form of the process, chronic and acute mesenteric intestinal thrombosis are distinguished. It can be localized only in the veins, only in the arteries, or have a mixed type, in which blood flow is first disrupted in the mesenteric arteries, and then in the venous vessels. Medical statistics indicate that the upper sections of blood vessels suffer from blockage more often than the lower ones.
Based on the degree of disruption of collateral blood flow and main arteries, it is customary to distinguish 3 main stages of the disease:
This stage is considered chronic intestinal ischemia. Blood flow in which is carried out due to unaffected vessels.
Partial blood supply to the intestines;
An extremely difficult stage, which in most cases is characterized by irreversible consequences. The blood supply to the intestines is completely absent, which causes a heart attack. Its first phase is only no more than 120 minutes.
At this time, there is still a chance for the process to be reversible. After 4 hours, the second phase begins, in which gangrenous damage to the organ rapidly develops.
This stage in most cases ends in death.
How does the blood supply work?
Arteries and veins are located almost parallel. Two large vessels depart from the abdominal aorta: the superior and inferior mesenteric arteries. They completely supply the intestines with blood.
The blood supply pattern is distributed as follows:
| Superior mesenteric artery | Inferior mesenteric artery |
| Transverse colon (70%) | Transverse colon (30%) |
| Cecum | Descending colon |
| Rising | Sigmoid |
| Small intestine | Rectum |
In 90% of cases, mesenteric thrombosis is observed in the superior mesenteric artery, in 10–15% of cases the masses close the lumen in the inferior artery.
Emboli can close the lumen of the mesenteric artery by entering it from the heart (if a mural thrombus breaks away), from the thoracic and abdominal aorta, or in the event of injury.
Thrombotic masses can also form in the veins. Their formation is caused by inflammatory processes in the intestines, congestion in the underlying vessels, and any other factors that increase blood viscosity.
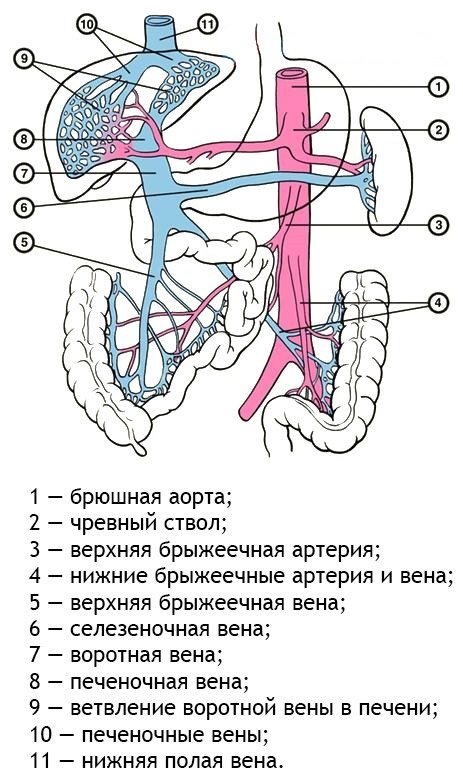
Blood supply to the intestines
Other causes of thrombosis
Almost any disease in which internal bleeding is possible is fraught with the formation and separation of blood clots, and therefore there are other reasons for the development of thrombosis of the mesenteric vessels.
These include:
- Severe intestinal infections;
- Portal hypertension with stagnation of blood in the portal vein;
- Injuries;
- Tumors compressing intestinal vessels.
What are the types of ischemia with mesenteric thrombosis?
In medical practice, there are three degrees of severity of the disease. They depend on the diameter of the mesenteric vessel lesion and the disruption of collateral flow.
- The decompensated form is the most severe stage. A time period of up to 2 hours is a reversible time when blood supply can be restored. The interval from 4 to 6 hours is partially reversible, the prognosis is not always favorable, deterioration can occur at any time, since the arterial and venous blood flow is completely disrupted. Over 6 hours, intestinal gangrene is observed.
- Subcompensated circulatory disorder - this form can be confused with other diseases. Acute vascular insufficiency is expressed by similar symptoms.
- The compensated degree is chronic ischemia, in which the function of blood flow is taken over by collaterals.
Forms and stages of development
The clinical picture of the condition includes three stages of its development:
- Ischemia with severe symptoms - pain, vomiting, frequent loose stools.
- Intestinal infarction with symptoms such as: constipation, severe pain, bloating, pale skin and bluish tint to the lips.
- Peritonitis is severe intoxication due to inflammation of the peritoneum with high fever, severe pain and tension in the abdominal wall.
The classification of thrombosis at the ischemic stage also includes several forms and types of severity:
- Decompensation is complete ischemia, the most severe form of the disease, progressing over a couple of hours.
- Subcompensation - there is collateral blood flow, the overlap is not complete.
- Compensation is a chronic form, the main blood flow is carried out through collaterals.
Symptoms of mesenteric thrombosis
Signs of thrombosis depend on the level at which the mesenteric arteries are blocked and on the form of intestinal ischemia.
Clinical manifestations are characterized by the following symptoms:
- The patient suddenly feels severe and acute pain ; it occurs in a subcompensated form. In the case of a decompensatory form of the disease, the painful sensations weaken and an imaginary improvement occurs, which is explained by the death of nerve endings (not a single artery supplies the intestines with blood);
- Manifestations of peritonitis - during palpation, tense muscles are felt, the abdomen is tight and swollen;
- Patients have impaired defecation - at the initial stage of the subcompensated form, loose stools are likely, in which impurities of blood and mucus are visible. With decompensation, tissue necrosis is observed, intestinal motility disappears and stool disappears;
- Intoxication of the body - observed if the patient has gangrene (the prognosis in most cases is unfavorable). This symptom is characterized by vomiting, nausea, low blood pressure;
- A state of shock - a person’s lips turn blue and their skin turns pale, there is an increased heart rate and a thread-like pulse.
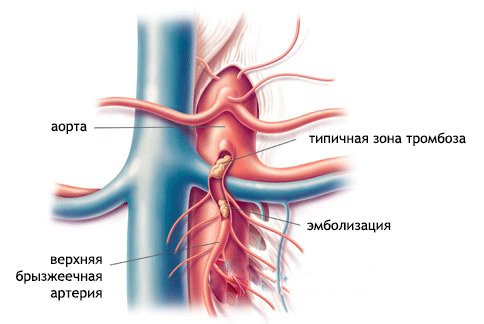
Thrombus zone
Treatment
If mesenteric thrombosis in the ischemic stage is suspected, conservative treatment can be carried out. Signs of intestinal necrosis and peritonitis require emergency surgical intervention.
Preparing for surgery
Before surgery for acute mesenteric thrombosis, it is necessary to empty the bladder and stomach. It is mandatory to stabilize the patient’s condition, replenish the deficit of blood volume, strive to normalize cardiac output, and stop bleeding. It is preferable to use Dopamine and Dobutamine as inotropic support. Preparation should not take more than 1-2 hours. The manipulations are performed under general anesthesia with mechanical ventilation.
Surgery
All operations for ischemia of the main branches of the intestine are divided into 4 types:
- vascular interventions;
- bowel resection;
- a combination of bowel resection and vascular intervention techniques;
- for peritonitis - intestinal resection, laparostomy, formation of sutureless enterostomies, programmatic sanitation of the abdominal cavity.
The most gentle and optimal method of treating thrombosis of the mesenteric arteries is endovascular thromboembolectomy under X-ray control. This is done in this way:
- antegrade recanalization;
- selective thrombolysis;
- aspiration thromboextraction;
- balloon plastic;
- stenting.
After endovascular access, heparin should be titrated at a rate of 1000 U per hour over the course of 24 hours.
Another surgical intervention to restore blood flow in the absence of endovascular access is open restoration of blood circulation. After laparotomy access, the small intestine is brought out into the wound, its mesentery is straightened, the site of thrombosis is determined by pulsation, and thromboembolectomy is performed through an arteriotomy hole or with a Fogarty catheter. Then the drug Actilyse is delivered distally for thrombolysis.
At the stage of infarction, intestinal resection with vascular intervention and program laparotomy are indicated. The main condition in case of a heart attack is that it makes no sense to form a primary anastomosis, since re-development of ischemia is likely.
In case of mesenteric vein thrombosis at the initial stage, blood flow can be restored using thrombolysis. If thrombosis is complicated by peritonitis, then part of the small intestine is removed.
Postoperative therapy
- During this period, patients are prescribed anticoagulants - Heparin 450 units per kg under the control of aPTT and thrombin time for 7-10 days, or Clexane 1 mg/kg 2 times a day for 6-14 days. After completion of treatment with direct anticoagulants, Warfarin is prescribed under the control of INR, the target value of which is 2-3.
- Antiplatelet agents are indicated when it is impossible to monitor the INR. Antibacterial therapy most often comes down to the use of Metronidazole and Ciprofloxacin, or a combination of Cefepime and Metronidazole in the development of peritonitis.
- After the operation, food is prohibited for 1-2 days. After the 2nd day, early tube feeding is prescribed to maintain the integrity of the gastrointestinal tract. Energy and electrolyte balance is maintained by parenteral nutrition.
- Be sure to provide adequate pain relief with prolonged epidural analgesia and narcotic analgesics.
- Ventilators are used if necessary.
- Plasmapheresis and hemodiafiltration to combat toxins.
- Restoring the amount of albumin in case of its deficiency.
Diagnostics
The sooner an accurate diagnosis is made, the greater the chance of a positive treatment outcome for the patient. The doctor needs to collect an anamnesis of the disease, ask the patient about the nature and time of onset of pain, and the frequency of stool. This will help determine the choice of surgical treatment.
The blood test shows pronounced leukocytosis (more than 20 * 109 l). Abdominal x-ray shows small bowel fluid levels.
The main diagnostic methods are:
- Laparoscopy is one of the decisive methods; it allows you to quickly examine the intestines, establish mesenteric obstruction and determine the stage of ischemia, because the surgeon has no more than two hours in reserve;
- Ultrasound of the abdominal organs - the procedure helps in differential diagnosis to exclude the possibility of other diseases;
- Selective angiography is a procedure that determines the levels of arterial occlusion and is necessary to provide emergency care. But many surgeons agree that it is inappropriate to spend time on angiography; if the course progresses rapidly, mesenteric thrombosis will end in death.

Intestinal laparoscopy
If it is not possible to perform laparoscopy, then surgeons perform laparotomy - an operation during which a large incision is made in the midline of the abdomen.
During the laparotomy process, doctors perform the following manipulations:
- The vessels are palpated to determine the location of the thrombus (each mesenteric artery and vein should be examined by the surgeon);
- The boundaries of viable intestinal tissue are identified;
- Completely examine the abdominal organs, assessing their condition;
- The pulsation of the arteries is detected, establishing the state of the blood supply to the intestines.
Staged symptoms of thrombosis
Ischemia
Thrombosis of mesenteric vessels begins acutely:
- Paroxysmal or constant abdominal pain;
- Vomiting mixed with bile already on the first day from the onset of the disease;
- Diarrhea.
These symptoms are very similar to the course of ordinary food poisoning, and therefore a visit to the doctor is often delayed.
Heart attack
When the vessels of the mesentery rupture under the pressure of blood trying to push out the thrombus, the stage of infarction occurs.
Diarrhea gives way to constipation, as deep pathological changes begin in the intestinal walls, and blood appears in the stool. Usually there is not a lot of it: heavy bleeding is not typical for mesenteric thrombosis.
If blood accumulates in the intestinal loops, patients may feel a small lump below the navel, which in medicine is called Mondor's sign.

The pain in the abdomen can be so unbearable that shock develops: patients are very restless, cannot find a place for themselves, and scream. Severe pallor and cyanosis of the lips are noted. Sometimes blood pressure may increase by 40-60 units (with thrombosis of the upper artery).
The rupture of the vessel brings temporary relief to the patient: the person calms down, since the intensity of the pain noticeably decreases, but vomiting and stool disorders persist.
The abdomen remains moderately swollen and soft, the characteristic phenomena of peritonitis (muscle protection and Shchetkin’s symptom) are not observed. The diagnosis of mesenteric thrombosis of intestinal vessels is made on the basis of ultrasound data and changes in the blood picture, which are expressed in a sharp increase in the number of leukocytes: this figure can reach 40•109 /l. The general blood test data shows a shift in the leukocyte formula to the left and high ESR numbers.
Peritonitis
Symptoms of peritonitis with thrombosis of intestinal vessels manifest themselves in a very unique way: tension in the muscles of the anterior abdominal wall and Shchetkin’s symptom are delayed, and the inflammatory process begins from below.
Developed intestinal paresis leads to the cessation of diarrhea and gas discharge.
Differential diagnosis
Mesenteric thrombosis is easily confused with other diseases, which is associated with a vague clinical picture.
The pathology is similar to the following diseases:
- Acute pancreatitis;
- Acute cholecystitis;
- Appendicitis;
Similar symptoms are characteristic of acute intestinal obstruction.
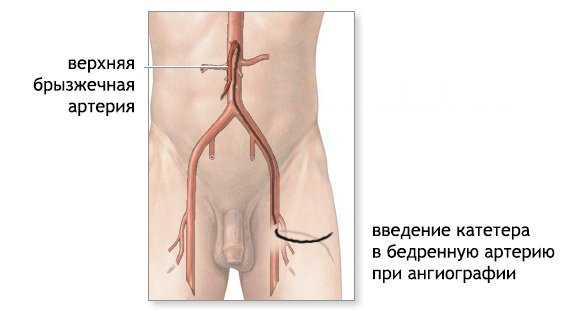
Diagnosis of mesothrombosis - insertion of a catheter
How is mesothrombosis treated?
The disease is amenable to surgical treatment only. The operation is performed under endotracheal anesthesia. At the first signs of pathology, the patient requires emergency care.
Antispasmodic and painkillers erase symptoms and make diagnosis difficult, which delays the possibility of surgery and leads to death.
Surgical intervention consists of important, mandatory parts:
- The surgeon examines the intestines, palpates the mesenteric vessels;
- The doctor must determine the pulsation in the arteries located at the borders of the affected intestines.
During the operation, the surgeon, if necessary, performs a resection - removes a section of necrotic intestine, then sutures the upper and lower borders.
If there are no necrotic changes yet, then the doctor must find a way to restore blood supply to the intestines and relieve ischemia from the affected area.
Restoring blood supply can occur in two ways:
- The surgeon gently squeezes the blood clot out of the vessels (artery or vein) with his fingers;
- A bypass shunt is created between the extreme boundaries of the thrombosed area.
During the recovery period after surgery, the patient is prescribed anticoagulants and blood thinners (“Heparin”). Therapy with these drugs is carried out under regular monitoring of the thrombosed index and INR.
If the necrotic part of the intestine is removed (for example: part of the ascending or small intestine), and normal blood supply is not restored, then in 80% of cases the situation ends in death.
Prognosis and complications
With the development of thrombosis, destruction primarily affects the mucous membrane, ulcers form, and signs of necrosis appear. If treatment is not started at this stage, tissue breakdown occurs. The intestinal wall is destroyed, resulting in the contents entering the abdominal cavity. Inflammation develops, which can be fatal.
Thrombosis of the intestinal mesenteric vessels is a dangerous disease that can lead to the development of severe consequences. When providing assistance in the early stages of the disease, the patient's condition stabilizes within a few days; in the case of late surgical intervention, the prognosis worsens. If treatment is not timely, complications develop in almost all patients. That is why it is important to consult a doctor when the first symptoms appear, who will prescribe the necessary measures to diagnose intestinal thrombosis and carry out treatment.
Forecast
The disease is detected during operations much more often than is registered. The fact is that the clinical picture of mesenteric thrombosis is similar to many other pathologies. It disguises itself as appendicitis, cholecystitis, or intestinal obstruction . There is not always enough time to make the correct diagnosis.
According to pathologists, mesenteric thrombosis accounts for up to 2.5% of cases. If the operation was performed within the first hours from the moment the blood clot occurred, then there is a high probability of recovery.
If surgery was performed after 12 hours, then the probability of death is up to 90%.