Surgical treatment of rectal cancer
Currently, clinical oncologists set the main goal of treatment for patients with rectal cancer to be complete recovery.
At the same time, they try to preserve the function of controlled defecation, so the approach of the patient from a number of specialists who combine the indicated methods of antitumor effects is important. The main treatment method for cancer of the final sections of the large intestine is surgery. It is usually supplemented with chemotherapy and radiation therapy .
Radical interventions for malignant tumors of the rectum are aimed at their removal, involving regional (nearby) lymph nodes. The choice of method is determined by the stage of the oncological process and the distance of the tumor from the anus. The constitutional characteristics of the patient, the presence and severity of concomitant pathology are also important.
Rectal tumors are common among general oncological pathologies, occupying first place in the structure of morbidity. At one time, the constantly increasing frequency of their occurrence led to closer attention.
In this regard, the following unified classification for rectal cancer was developed. It includes not only the appearance of symptoms, but the anatomical and morphological features of the tumor process.
Determining the stage of the disease according to the TNM7 system (2009) serves as the main way to select the volume and type of surgery. It includes the following parameters:
| Stage | T | N | M |
| 0 | is | 0 | 0 |
| I | 1,2 | 0 | 0 |
| II (A,B,C) | 3,4 | 0 | 0 |
| III (A,B,C) | any | 1,2 | 0 |
| IV (A,B) | any | any | 1 |
Planning of surgical treatment is carried out after establishing a diagnosis in accordance with the nosological form according to ICD-10 (international classification of diseases). This is only possible with a histological examination of the material obtained from a colon or surgical biopsy (a study of the metastatic lesion is also carried out).
If the tumor is located less than 15 cm from the anus (determined using a rigid proctoscope), it is classified as rectal.
Diagnostic minimum
In the preoperative period, the patient is examined in the following scope:
- Assessment of anamnestic data, physical examination;
- General and biochemical blood tests with assessment of liver and kidney function indicators;
- Determination of levels of tumor markers CEA, CA 19-9 and others as prescribed by a doctor;
- Recto-, colon- and/or irrigoscopy with biopsy;
- Ultrasound, CT/MRI (at least 1.5 T) of the abdominal organs;
- X-ray/CT scan of the chest (to assess the presence of distant metastases);
- Transrectal ultrasound/MRI of the pelvic organs (determine the depth of invasion and involvement of regional lymph nodes).
Diet
To properly prepare for surgery, you need to adjust your diet 2-3 weeks (if possible) as follows:
- It is necessary to eat food in fractional mode - in small portions, at regular intervals, 5-6 times a day;
- Avoid fatty, smoked, overly salted, spicy, spicy or grilled foods;
- Limit the consumption of milk, hard cheeses, mushrooms, nuts, coffee, strong tea, semolina and rice porridge;
- Various fermented milk products, vegetables and fruits in any form are introduced into the diet;
- White bread is replaced with bran or rye flour;
- Every day you need to consume at least 2 liters of water, including compotes, uzvar, first courses in low-fat broth;
- It is recommended to eat porridge made from buckwheat, pearl barley, oatmeal with the addition of dried fruits (prunes, raisins, dried apricots);
- Food is steamed, boiled or baked under foil.
After fulfilling all the requirements, the patient is hospitalized in the inpatient department, where further preparation will be carried out by medical staff.
Types of surgical interventions
Performing surgery at an early stage allows you to prolong the patient’s life for decades, achieving full recovery in most cases. The more severe the tumor progression, the more extensive and complex the surgical intervention.
Surgery for rectal cancer can be performed in the following ways:
- Endoscopic;
- Radical.
Endoscopic treatment
The following indications for endoscopic treatment of tumor diseases of the rectum are distinguished:
- The presence of adenomas with epithelium in a state of severe dysplasia (cellular mutations);
- For adenocarcinoma of the rectum with invasion up to the submucosal layer (according to ultrasound/MRI);
- Tumor
- No more than 30% of the intestine in diameter is affected;
- Education is fluid.
A polypectomy or submucosal resection of an area of the rectum with severe cellular dysplasia is performed.
The use of an endoscopic treatment option is associated with the risk of relapse or the development of complications in the early postoperative period (pain, bleeding or intestinal perforation).
Radical operations
If the tumor is localized less than 6-7 cm from the anus, the rectum is removed using the abdominoperineal method. In more distant locations, it is possible to preserve the sphincter when performing resection (part of the organ is partially removed).
Surgery to remove rectal cancer is performed in the following ways:
- Abdominoperineal extirpation of the rectum (Quenu-Miles operation);
- Anterior rectal resection;
- Abdominal-anal resection of the rectum;
- Hartmann's operation;
- Palliative operations.
Abdominoperineal extirpation
This type of intervention involves removing the entire rectum with part of the sigmoid and colon. After this, a single-barrel colostomy is placed in the left lower abdomen (iliac region).
The operation consists of the following steps:
The intervention begins with a lower median laparotomy to mobilize the sigmoid and rectum with the formation of a colostomy. After this, the wound on the anterolateral abdominal wall is sutured. Next, the straight line is removed, leaving drainage in the precoccygeal (presacral) space.
By “mobilization” we should understand the removal of a part of an organ to work with it. In this case, they usually tie (ligate) or temporarily apply clamps to the neurovascular bundles.
Anterior resection
Surgery for rectal cancer in the form of anterior resection is also performed through a lower median laparotomy. The following steps are carried out:
- Mobilization of the rectum and its intersection 4-5 cm below the tumor;
- Suppression of the colon with anastomosis with the rectal stump;
- A drainage is left in the presacral space, and a probe is inserted into the intestine through the anus.
Abdominoanal resection
During this operation, the sigmoid part of the colon is reduced after a median laparotomy. Next, mobilize the direct line and perform the following actions:
- The anal canal is stretched with dissection along the posterior rectal line;
- The mucous membrane above the anal canal is separated, after which the rectum is cut off;
- The rectum and sigmoid parts of the intestine are brought down at the shown level through the anus, and their edges are fixed along the perimeter of the anal canal.
In some cases, surgeons refuse to excise the mucous membrane of the anal canal, making an anastomosis (communication) between the reduced colon and the remaining part of the rectum.
Hartmann operation
The Hartmann operation is performed very similarly to previous techniques. Surgeons act according to the following algorithm:
- Access – lower median laparotomy;
- Mobilization of the sigmoid, colon and rectum;
- Transection of the rectum below the location of the tumor, suturing its stump;
- Cutting off the affected section;
- Application of a single-barrel colostomy in the left iliac region.
Palliative operations
These types of operations, as the name suggests, are aimed at temporarily prolonging the life of a patient in severe stages of cancer, which will reduce his suffering.
Palliative interventions are carried out in the presence of severe symptoms of intestinal obstruction or the impossibility of radical treatment. The choice of the extent of the operation is usually left to the discretion of the oncologist.
More often, a double-barreled colo- or sigmostoma is applied with its removal on the anterolateral wall of the abdomen on the left.
Schemes of operations
Surgeries for rectal cancer are carried out according to the established stage of the disease according to the following scheme:
| Stage | Scope of operation | Other treatments |
| T0 |
| Observation. |
| T1-2 |
| Observation. |
| T3-4 |
|
|
The criterion for successful radical intervention is the survival of patients over the next 5 years after surgery (and/or other types of treatment). For rectal cancer, it averages about 40-50%. But it should be taken into account that patients come in at late stages, which significantly affects the indicators.
Rectal cancer is dangerous because it can be completely asymptomatic in the first stages or “masquerade” as other diseases - hemorrhoids, syphilis, endometriosis, sarcoma, villous tumor. However, this does not exclude the simultaneous presence of several pathologies.
The situation is much more favorable when performing surgical treatment at stages I-II of a tumor disease, as well as with exophytic cancer (growing into the intestinal lumen) with a high degree of differentiation (maturity) of cells.
Carrying out an operation always involves certain risks. In some cases, the following consequences may develop:
- Attachment of a secondary infection (usually in the area of a wound or colostomy);
- Bleeding;
- Extending the period of tissue repair (restoration) in weakened patients, as well as with multiple concomitant pathologies;
- Dehiscence of postoperative sutures;
- Peritonitis;
- Various types of digestive disorders (constipation, diarrhea, flatulence);
- Fecal or urinary incontinence;
- Erectile dysfunction up to impotence;
- Adhesive process in the abdominal cavity.
A worse prognosis should be expected in young patients, in particular with anal cancer.
Rehabilitation and clinical observation
In the postoperative period, depending on the stage of the cancer, the patient is observed or undergoes additional treatment (chemo- or radiation therapy) to achieve the effects of complete remission.
Rehabilitation includes adherence to the general principles of postoperative recovery. As a rule, patients are recognized as disabled for an indefinite amount of time (depending on the volume of intervention, age, stage of the process).
The postoperative period involves compliance with the following recommendations:
- For the first 1-3 days after the operation, you will not be able to eat, only drinking mineral still water is allowed;
- For the entire period of hospital stay - gentle food (semi-liquid porridges, pureed soups);
- Wearing a bandage to reduce the load on the abdominal muscles (prevents a sharp increase in pressure in the abdominal cavity);
- When applying a colostomy, follow the instructions of the doctor or special instructor for its care;
- After discharge, diet No. 4 with the addition of indicated medications;
- Moderate activation of the patient.
The main goal of the rehabilitation period is to prevent complications in a hospital setting and explain to the patient the need for further clinical observation. In some cases, consultation with a psychologist may be required.
After completion of treatment, it is recommended to follow the following observation plan:
- During the first 2 years, regular physical examinations by the treating oncologist are performed every 3-6 months. In the next 3-5 years - once every 6-9 months;
- After 5 years from the date of the operation, they are observed once a year or when characteristic complaints appear;
- The following examinations are carried out periodically:
- Digital examination of the rectum;
- Determination of tumor markers in blood serum every 3 months for the first 2 years and subsequently once every 6 months;
- Colonoscopy after 1 and 3 years, then every 5 years, if polyps are present - annually;
- Ultrasound examination of the abdominal and pelvic organs every 3-6 months (depending on the risk of progression or relapse);
- Chest X-ray annually/CT with intravenous contrast once 18 months after surgery for rectal cancer.
Clinical observation is necessary for early detection of cancer progression with the aim of timely initiation of polychemotherapy courses or other surgical treatment options (including metastatic foci or tumor recurrence).
Source: https://easymed-nn.ru/zabolevaniya/onkologiya/operaciya-na-pryamoy-kishke.html
Consequences after rectal surgery
The rectum is the final segment of the human digestive tract and performs a very important function: feces are accumulated and excreted here. The normal functioning of this organ is very important for a full, high-quality human life.
The main diseases of the rectum: hemorrhoids, rectal prolapse, anal fissure, proctitis, paraproctitis, ulcers, benign and malignant tumors.
The most significant and most complex operations on the rectum are operations for oncological diseases of this organ.
Precisely because feces accumulate in the rectum, its mucosa has the longest contact with digestive waste compared to other parts of the intestine. This explains the fact that the largest percentage of all intestinal tumors are rectal tumors.
The radical treatment for rectal cancer is surgery. Sometimes surgical treatment is combined with radiation therapy, but if a rectal tumor is diagnosed, surgery is inevitable.
The rectum is located mostly in the small pelvis, deep, which makes it difficult to access. Through a conventional laparotomy incision, only tumors of the supramullary (upper) part of this organ can be removed.
Types of rectal resections
The nature and extent of the operation depends on the location of the tumor, or more precisely, the distance from the lower edge of the tumor to the anus, on the presence of metastases and on the severity of the patient’s condition.
If the tumor is located less than 5-6 cm from the anus, abdominal-perineal extirpation of the rectum is performed, that is, its complete removal along with the surrounding tissue, lymph nodes and sphincter.
During this operation, a permanent colostomy is formed - the descending sigmoid colon is brought out and sutured to the skin in the left half of the abdomen.
The unnatural anus is necessary for the removal of feces.
In the first half of the 20th century, when rectal cancer was detected, only its removal was performed.
Currently, the approach to radical treatment of tumors of this organ has been revised in favor of less mutilating operations. It has been found that complete removal of the rectum is not always necessary. When the tumor is localized in the upper or middle third, sphincter-preserving operations are performed - anterior resection and abdominal-anal amputation of the rectum.
The main types of rectal operations currently used:
- Abdominoperineal extirpation.
- Anterior rectal resection.
- Abdominal-anal amputation with reduction of the sigmoid colon.
In cases where it is impossible to radically remove the tumor, a palliative operation is performed to eliminate the symptoms of intestinal obstruction - a colostomy is removed, and the tumor itself remains in the body. Such an operation only alleviates the patient’s condition and prolongs his life.
Anterior rectal resection
The operation is performed when the tumor is located in the upper part of the intestine, on the border with the sigmoid. This section is easily accessible through the abdominal approach. The intestinal segment along with the tumor is excised and removed, the descending segment of the sigmoid and the rectal stump are sutured manually or using a special device. As a result, the sphincter and natural bowel movements are preserved.
Other treatments
- For tumors larger than 5 cm and suspected metastasis to regional lymph nodes, surgical treatment is usually combined with preoperative radiation therapy.
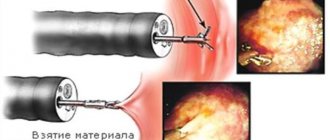
- Transanal tumor resection. It is carried out using an endoscope in cases of small tumor size (no more than 3 cm), its germination no further than the muscle layer and complete confidence in the absence of metastases.
- Transanal resection of part of the rectum.
- It is also possible to perform laparoscopic resection of the rectum, which significantly reduces the invasiveness of the operation.
Contraindications for rectal surgery
Since surgery for malignant tumors is a life-saving operation, the only contraindication to it is the very serious condition of the patient.
Quite often, such patients actually arrive at the hospital in serious condition (cancer cachexia, anemia), but preoperative preparation for some time makes it possible to prepare such patients.
Source: https://okishechnike.com/info/posle-operacii-na-prjamoj-kishke-posledstvija/
How are they treated?
The method of treatment for rectal cancer is determined depending on the patient’s condition, location and size of the tumor. The central method of treatment is surgery. But at stages 3-4 it is not enough, and an integrated approach is used:
- Radiation therapy before and after surgery;
- Surgical intervention;
- Polychemotherapy.
Comprehensive treatment greatly increases the chances of recovery.
On average, rectal cancer surgery costs:
- in Israel - from $20,000;
- in Germany - from € 15,000;
- in Russia - from 20,000 rubles.
How is surgery performed for rectal cancer and possible consequences?
The appearance of growths on the intestinal walls is associated with the development of a tumor. At the initial stage, the neoplasm is benign, but due to provoking factors it becomes an oncological manifestation.
If conservative treatment was not provided on time, then the patient needs surgery for rectal cancer.
To remove a malignant tumor, there are several methods of performing a surgical procedure.
Clinical manifestations and stages of tumor in the rectum
In order not to confuse cancer in the rectum (rectum), you need to know the symptoms, and then treatment is prescribed. When a malignant tumor appears, the patient experiences a general loss of strength and insomnia. Appetite gradually decreases and bone pain occurs. Poor nutrition causes dizziness.
A patient with a malignant growth in the rectum may not notice an increase in body temperature to 37°C. This symptom begins to appear constantly.
The patient begins to feel and cannot tolerate any odors, and blood and mucus are present in the stool. When the formation in the rectum continues to develop, the pain syndrome manifests itself in the following places:
- sacrum;
- coccyx;
- crotch.
During the act of defecation, feces come out in the form of a ribbon. The patient complains of a frequent urge to have a bowel movement and a feeling of a foreign body in the rectum. This contributes to constipation.
Symptoms appear as a certain stage of the disease progresses. Therefore, the initial stage is characterized by a tumor within the mucosal epithelium. The lesion occupies a small area and does not metastasize.
The next stage is accompanied by an increase in growth up to 5 cm. At this stage, metastases to nearby lymph nodes may be observed. The third stage is characterized by the tumor size exceeding 5 cm. Metastases are present in the lymph nodes. At the final stage, the neoplasms move to other organs and systems. Metastasis occurs to other tissues and lymph nodes.
Therapeutic methods
The initial stages of a tumor located in the rectum can be cured with surgery. The use of radiation and chemotherapy will not help get rid of the disease. Therefore, treatment is carried out comprehensively. Special therapy is carried out before and after surgery to remove rectal cancer.
Surgical procedures for the treatment of oncology
Intervention to remove a tumor in the rectum is not performed if the patient is admitted to the surgeon in serious condition. In addition, for certain diseases, surgery for rectal cancer is not performed due to a weakened body. In other cases, depending on the diagnostic indications, cancer treatment methods are carried out with complete or partial removal of the rectum.
With anterior resection, doctors remove the growth when the growth is located in the upper part of the rectum. The intervention occurs in the form of an incision in the lower abdomen and the connection between the sigmoid colon and the rectum is removed. Low resection is done when the tumor is in the middle or lower parts of the rectum. The surgeon performs a complete removal of the rectum.
Extirpation of the patient occurs with two incisions, located in the abdomen and perineum, when the cancer affects most of the rectum. The patient's rectum, areas with growths in the anal canal, and nearby tissue are removed.
Local removal is performed for grade 1 tumors using an endoscope. The procedure allows you to remove small growths in the rectum. If the formations are located near the anus, then the endoscope is not used. The tumor is removed by inserting surgical instruments through the anus.
In addition to resection, surgery uses methods to remove the tumor while preserving the sphincter. In this case, transanal excision may be performed. The indication for surgery is the appearance of tumors in the lower part of the rectum. Special surgical instruments are used for the procedure. In this case, the lymph nodes are not removed.
The surgeon may use open laparoscopy. This requires making several incisions in the abdominal wall. A laparoscope is inserted into one hole, surgical instruments are inserted into the others and growths or the affected area are removed. Laparoscopic resection allows the patient to recover quickly after surgery.
Preparatory activities for the patient
Before surgery, the patient is prepared for the procedure. The patient is advised to consume a minimum amount of fiber foods. The attending physician discontinues medications that thin the blood. Instead, antibacterial drugs are prescribed.
The day before surgery, you will need to drink more fluids, but you should not eat solid food. This allows you to easily cleanse the intestines.
Forced bowel movements can be done in several ways. Cleansing enemas are suitable for this, which are done throughout the day at regular intervals. If necessary, strong laxatives are used, and 8 hours before the procedure it is forbidden to eat or drink liquids.
If the patient is admitted in a weakened state, then surgery to remove the tumor in the rectum is postponed. In a hospital setting, they receive a blood transfusion. Doctors prescribe intravenous administration of the necessary solutions. After normalization of the condition, surgery is permitted. The surgical treatment takes over 3 hours. Removal of growths takes place under general anesthesia.
How is the recovery process after surgery going?
When complete extirpation of the rectum is performed, surgeons create a stoma at this site. Doctors should warn about performing and creating an artificial anus. This fact becomes the reason for refusing to perform extirpation.
After surgery, you must follow your doctor's recommendations. The patient spends several days in the hospital. Postoperative stay in the hospital allows you to normalize digestion and body processes.
An oncologist prescribes medications. If the patient has a colostomy, then they explain to him how to live with this device. In modern medicine, the hole can be secured with plates that adhere to the skin.
In addition, methods and means for stoma care are discussed.
Possible complications after removal of growths
Unpleasant consequences can occur not only before treatment, but also after surgery. Due to the complexity of the process, rectal extirpation can result in complications for the patient.
The consequences include the following:
- incomplete removal of tumors;
- damage to nerve endings;
- damage to other organs.
Therefore, the patient may be at risk of tumor recurrence. Otherwise, problems with urination arise when the patient does not control the process of emptying the bladder. Sometimes internal bleeding occurs.
Recommendations for discharge from hospital
When treatment for colon cancer is completed and the patient is at home, he needs to care for the stoma. After tumor removal, therapy continues, which consists of normalizing nutrition. Doctors recommend following a diet for cancer.
Nutritional correction for rectal cancer is the same, both before and after the procedure. Therefore, meals are consumed in small portions up to 6 times a day. The menu should include fermented milk products. Vegetables and fruits from which purees or salads are made are considered healthy.
Buckwheat, pearl barley and oatmeal help improve digestion. It is allowed to eat lean meat and seafood. Dishes should be served boiled or steamed.
Over time, dietary therapy begins to be violated, which leads to problems with the digestive tract.
If loose stools appear after tumor surgery, then you need to remove low-fiber foods from your diet. When the rehabilitation period ends and digestion returns to normal, the patient can switch to regular foods. To do this, you should consult a nutritionist.
In addition to nutrition, when surgery is performed for a rectal tumor, the patient is given exercises. They are necessary to strengthen the muscles of the rectum and sphincter.
If symptoms of a growth in the intestines are detected, timely assistance should be provided. Otherwise, you will need to treat the consequences of a rectal tumor, which can be fatal.
Oncological formations in the rectum are accompanied by pain and the release of pus and mucus from the anus along with feces.
At the initial stages, growths are removed without total removal of the rectum.
The information on our website is provided by qualified doctors and is for informational purposes only. Don't self-medicate! Be sure to consult a specialist!
Rumyantsev V. G. Experience 34 years.
Gastroenterologist, professor, doctor of medical sciences. Prescribes diagnostics and carries out treatment. Expert of the group for the study of inflammatory diseases. Author of more than 300 scientific papers.
Doctor We recommend: What is chronic appendicitis: signs in men and women
Source: https://gastrot.ru/kishechnik/opuhol-pryamoj-operatsiya-i-posledstviya
Causes of tumors in the intestine
A predisposition to mutational changes in cells in the intestinal mucosa is noted after exposure to carcinogenic substances that enter the body with food. Such substances are mainly components of fried foods, smoked products and synthetic ones. Some food products contain substitutes for natural taste, smell and color, which negatively affect the digestive process and the functionality of the stomach and intestines. A monotonous and unbalanced diet, exhausting diets for weight loss, can also serve as a risk factor for inflammatory processes in the intestines with subsequent degeneration into cancer. The cause of oncology can be alcohol and drug intoxication, as well as poisoning with toxic substances of medicinal origin and after eating low-quality food.
The entry of carcinogens into the body can also be observed in workers in hazardous industries.
Intestinal cancer can occur with frequent congestion, constipation and slag deposits on the walls of the intestinal canals. Long-term constipation not only increases carcinogenic levels, but also has an irritating effect by putting pressure on the intestinal walls. Infectious diseases and chronic inflammatory processes of the intestinal system, such as:
- Peptic ulcer;
- Esophagitis and leukoplakia of the esophagus;
- Duodenitis;
- Colitis;
- Crohn's disease;
- Enteritis;
- Polyposis and adenomatosis;
- Pancreatitis.
Postoperative scars, polyps, diverticula, granulomas and infiltrates can also be precancerous conditions.
Not least in the etiology of intestinal cancer is genetic predisposition.
Surgeries on the rectum: indications, types, indications, prognosis
All materials on the site were prepared by specialists in the field of surgery, anatomy and specialized disciplines. All recommendations are indicative in nature and are not applicable without consulting a doctor.
The rectum is the final segment of the human digestive tract and performs a very important function: feces are accumulated and excreted here. The normal functioning of this organ is very important for a full, high-quality human life.
The main diseases of the rectum: hemorrhoids, rectal prolapse, anal fissure, proctitis, paraproctitis, ulcers, benign and malignant tumors.
The most significant and most complex operations on the rectum are operations for oncological diseases of this organ.
Precisely because feces accumulate in the rectum, its mucosa has the longest contact with digestive waste compared to other parts of the intestine. This explains the fact that the largest percentage of all intestinal tumors are rectal tumors.
The radical treatment for rectal cancer is surgery. Sometimes surgical treatment is combined with radiation therapy, but if a rectal tumor is diagnosed, surgery is inevitable.
The rectum is located mostly in the small pelvis, deep, which makes it difficult to access. Through a conventional laparotomy incision, only tumors of the supramullary (upper) part of this organ can be removed.
Preparing for rectal surgery
Basic examinations that are prescribed before surgery:
- Tests: general blood tests, urine tests, biochemical blood test, coagulogram, determination of blood group and Rh factor.
- Study of markers of infectious diseases - viral hepatitis, syphilis, HIV.
- Electrocardiogram.
- X-ray of the chest organs.
- Ultrasound examination of the abdominal organs.
- Examination by a therapist.
- For women - examination by a gynecologist.
- To more accurately determine the extent of the tumor, an MRI of the pelvic organs may be prescribed.
- A biopsy of the tumor is required to determine the extent of tissue removal (for less differentiated types of tumors, the boundaries of the tissue removed should be expanded).
A few days before surgery:
- A slag-free diet (with minimal fiber content) is prescribed.
- Drugs that cause blood thinning are discontinued.
- Antibiotics are prescribed to kill pathogenic intestinal flora.
- On the day before the operation, solid food is not allowed (you can only drink), and the intestines are cleansed. It can be done:
- With the help of cleansing enemas performed after some time during the day.
- Or taking strong laxatives (Fortrans, Lavacol).
- 8 hours before surgery, food and water are not allowed.
In cases where the patient is very weakened, surgery may be postponed until the general condition normalizes. Such patients undergo transfusion of blood or its components (plasma, red blood cells), parenteral administration of amino acids, saline solutions, treatment of concomitant heart failure, and metabolic therapy.
The rectal resection operation is performed under general anesthesia and lasts at least 3 hours.
Postoperative period
Immediately after the operation, the patient is placed in the intensive care unit, where the functions of the heart, breathing, and gastrointestinal tract will be carefully monitored for 1-2 days.
A tube is inserted into the rectum, through which the intestinal lumen is washed with antiseptics several times a day.
Within 2-3 days the patient receives parenteral nutrition, after a few days it is possible to take liquid food with a gradual transition to solid food over two weeks.
To prevent thrombophlebitis, special elastic stockings are put on the legs or elastic bandages are used.
To reduce tension in the abdominal muscles, it is recommended to wear a special bandage.
Painkillers and antibiotics are prescribed.
Main complications after rectal surgery
- Bleeding.
- Damage to neighboring organs.
- Inflammatory suppurative complications.
- Urinary retention.
- Dehiscence of anastomotic sutures.
- Postoperative hernias.
- Thromboembolic complications.
Life with a colostomy
If a complete extirpation of the rectum with the formation of a permanent colostomy (unnatural anus) is to be performed, the patient should be warned about this in advance. This fact usually shocks the patient, sometimes to the point of categorically refusing the operation.
Very detailed explanations are needed to the patient and relatives that a full life with a colostomy is quite possible. There are modern colostomy bags that are attached to the skin using special plates, are invisible under clothing, and do not allow odors to pass through. Special products for stoma care are also available.
When discharged from the hospital, ostomy patients are trained in stoma care, control of discharge, and a colostomy bag of the appropriate type and size is selected for them. In the future, such patients have the right to free colostomy bags and plates.
Diet after rectal surgery
For the first 4-6 weeks after rectal surgery, the consumption of coarse fiber is limited. At the same time, the problem of preventing constipation becomes urgent.
It is allowed to eat boiled meat and fish, steamed cutlets, stale wheat bread, soups with weak broth, porridges, vegetable purees, stewed vegetables, casseroles, dairy products, taking into account milk tolerance, pasta dishes, eggs, fruit purees, jelly. Drink – tea, herbal decoctions, still mineral water.
The volume of liquid is at least 1500 ml per day.
Gradually, the diet can be expanded.
The problem of preventing constipation is urgent, so you can eat wholemeal bread, fresh vegetables and fruits, rich meat broths, dried fruits, and sweets in small quantities.
Patients with a colostomy usually experience discomfort with excessive gas, so they should be aware of foods that can cause increased gas: milk, brown bread, beans, peas, nuts, carbonated drinks, beer, baked goods, fresh cucumbers, radishes, cabbage, onions and some other products.
The reaction to a particular product can be purely individual, so such patients are recommended to keep a food diary.
Possible complications
Since rectal resection is a complex operation, it is natural that various consequences may arise. Such complications are considered:
various infections; negative effects of anesthesia; hernia or bleeding; problems with urination; damage to other organs.

You should also consider factors that may increase complications after surgery. Doctors always inform patients about the reasons that may cause difficulties with resection and further recovery, for example:
infectious diseases; diabetes and smoking; overweight; the patient's age exceeds 70 years; heart and lung diseases.