Main symptoms:
- Pale skin
- Abdominal pain
- Pain in the anal area
- Constipation
- Change in heart rate
- Blood in stool
- Sleep disturbance
- Straining during defecation
- Feeling of fullness in the intestines
- Mood swings
- Increased gas formation
- Loss of appetite
- Rare urge to defecate
- Dry stool
- Hardness of stool
- Nausea
- Heaviness in the stomach
- Increase in abdominal volume
- Rumbling in the stomach
- Feeling disgusted by food
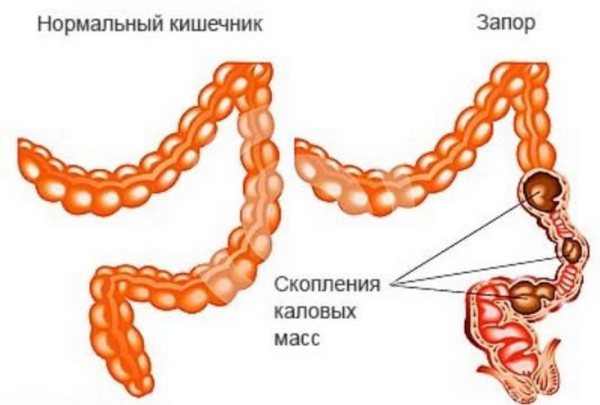
Coprostasis is fecal stagnation, which causes complete or partial blockage of the lumen of the large intestine. The disease develops in both adults and children. Treatment can only be prescribed by a doctor after diagnosis.
- Etiology
- Classification
- Symptoms
- Diagnostics
- Treatment
- Prevention and prognosis
The pathology almost never occurs as an independent disease, but progresses against the background of other gastroenterological or endocrinological anomalies. There are several physiological predisposing factors.
The fundamental external sign is the inability to independently carry out the act of defecation. The clinical picture includes pain, heaviness and rumbling in the intestines, changes in the general well-being of the patient.
The diagnostic process must necessarily take an integrated approach and include a wide range of laboratory and instrumental examinations, primary diagnostic manipulations carried out by a clinician.
Treatment of pathology begins with the use of conservative methods - taking medications and enemas. In cases of the formation of hard fecal stones, surgical intervention is indicated.
According to the international classification of diseases ICD-10, intestinal stagnation of feces has a separate meaning - code K59.0.
Etiology
A large number of unfavorable predisposing factors can cause the pathology. The most common triggers are diseases that negatively affect the intestines. Among them it is worth highlighting:
- IBS;
- intestinal dysbiosis and diverticula;
- dolichocolon, megacolon, dolichosigma and other pathological conditions that lead to an increase in the volume of some parts of the organ;
- the occurrence of inflammatory, infectious or pathological processes in a given localization;
- dysfunction of the intestinal sphincters.
Intestinal obstruction can be caused by diseases associated with other internal organs and systems:
- diabetes mellitus and other diseases of the endocrine system;
- metabolic disorder;
- peptic ulcer;
- pancreatitis;
- cholecystitis;
- gastritis;
- ulcerative colitis;
- external and internal hemorrhoids;
- diseases of the cardiovascular system and central nervous system;
- polyneuropathy;
- portal hypertension;
- poisoning;
- dehydration of the body.
Every person is susceptible to the disorder, and older people are no exception. In such situations, provocateurs can serve as:
- a completely normal aging process;
- the presence of a large number of chronic diseases;
- dysfunction of the nervous regulation of the intestines.
Coprostasis syndrome in children most often appears due to the following factors:
- enzyme deficiency;
- food allergies;
- congenital pathologies, for example, Hirschsprung's disease;
- lactose intolerance;
- purely childhood diseases, in particular rickets;
- prolonged refusal to eat;
- food that does not correspond to the child’s age category;
- stressful situations in the family, kindergarten or school.
Among female representatives, the condition is diagnosed more often. This is due to the influence of such specific reasons:
- hormonal imbalance that occurs during entry into the postmenopausal period;
- the period of intrauterine development of the fetus, during which the increasing size of the uterus, like the growing child, leads to compression and displacement of internal organs, which causes intestinal obstruction;
- the pursuit of an ideal figure, which forces women to adhere to strict diets;
- labor - provokes weakening of the pelvic floor muscles;
- the passage of critical days;
- overdose of hormonal drugs.
Sometimes coprostasis is formed against the background of physiological sources, i.e. those that do not have a pathological basis. This category of predisposing factors combines:
- alcohol and tobacco abuse;
- prolonged refusal to eat followed by overeating;
- ingestion of cold foods and drinks;
- drinking insufficient volume of liquid - a person needs to drink an average of 2 liters of water per day;
- psycho-emotional stress;
- physical fatigue;
- sedentary lifestyle.
It is noteworthy that the influence of genetic predisposition to the disease and the formation of fecal stones cannot be excluded.
Coprostasis
Intestinal obstruction in children under one year of age symptoms
After surgery for intestinal obstruction in a child at 5 years old or at another age, children are prescribed dietary nutrition for a long period. This forced measure helps normalize digestion and restore intestinal function. It has been proven that every fourth case of this disease is caused by poor diet.
It is important to remember that if the intestine is blocked (in the acute phase), any food intake is contraindicated for the baby. During the first days after the operation, they are also not fed, but on the second day they are given liquid food. For intestinal obstruction, doctors recommend:
- Eat small meals eight times a day.
- All food is ground to a pasty state and consumed warm.
- Calorie content during the first days is 600, up to 1000 kcal seven days after surgery.
The following products are allowed:
- jelly;
- jelly;
- porridge;
- mucous decoctions;
- spoiled milk;
- fruit jelly;
- low-fat poultry broth;
- pureed vegetables;
- omelette;
- steamed meatballs.
During the year, foods that cause fermentation are prohibited. In addition, salt intake is limited. Failure to adhere to the diet increases the risk of relapse of the disease.
What is intestinal obstruction and for what reasons does it occur in children?
Intestinal obstruction is a partial or complete disruption of the movement of digested food and feces through the intestines, associated with a malfunction in the motor function of the intestine or with the occurrence of a mechanical obstruction. Intestinal obstruction occurs:
- congenital – occurs due to abnormalities in the development of the intestinal tract;
- acquired, which, in turn, is divided into mechanical and dynamic.
Congenital intestinal obstruction in newborns is associated with abnormal fetal development or disease. The main symptom is the absence of stool, because it should appear in the baby immediately after birth. The baby's intestines in the womb are filled with fluid, which after the baby is born is released in the form of primary feces - meconium.
The acquired form is typical for older children, because it appears as a result of previous diseases. It occurs suddenly, and it is often possible to accurately determine the moment of onset of the pathology. Obstruction is accompanied by severe pain, bloating (usually asymmetrical), and vomiting.
There are other factors that contribute to the occurrence of pathology:
- violation of the infant's diet (early or too late introduction of complementary foods), inflammatory diseases of the intestinal tract;
- entry of a foreign body into the intestines;
- hardening of stool with the formation of stones caused by poor diet or digestive disorders;
- surgical interventions;
- volvulus.
All cases of intestinal obstruction are accompanied by severe symptoms. At the first suspicion of a pathology, you should consult a doctor.
Treatment of illness in a baby
If you notice signs of intestinal obstruction in a child, do not give him food or medicine until he has been examined by a doctor.
Emergency medical attention is required to avoid dehydration and severe shock, and to prevent infection that can occur when part of the intestine dies due to lack of blood.
The baby is examined for the presence of intestinal disease by a surgeon. If complications occur, surgical intervention is necessary.
To treat intestinal obstruction, your doctor may prescribe:
- Air enema or barium enema. It is both a diagnostic procedure and a treatment. If the enema works, further treatment is usually not required. This procedure is very effective in children.
- Surgery. If the intestines rupture or enemas fail to straighten the intestines, surgery is necessary. The surgeon will release the part of the intestine that has become twisted, remove the blockage (obstruction), and, if necessary, remove dead intestinal tissue.
If the intestinal disease is not in an acute, advanced stage, conservative therapy is prescribed. It consists of a set of procedures to remove stagnant feces from the intestines and cleanse the body of harmful substances and toxins.
The following procedures may also be prescribed to your baby:
- To stop the vomiting process, the stomach is lavaged through a special tube;
- Medicines are administered intravenously that help restore water-salt balance;
- Antiemetic, analgesic and antispasmodic medications;
- If treatment is successful, the baby may be prescribed the medicine proserin, which stimulates proper intestinal activity.
Complications and prognosis for the child
The worst complication of intestinal obstruction in a child is death. As the anomaly progresses, the body becomes intoxicated. The blood supply to the digestive organs is significantly disrupted, and as a result, the tissues of the intestinal wall are destroyed and die. Both toxins and water and nutrients stop entering the bloodstream.
In addition, there are other, less dangerous, but quite serious complications: kidney failure, severe dehydration, failure of vital systems.
If the contents of the intestine are stopped by a certain obstacle, the child’s body takes more fluid from the intestinal lumen than it should. The tummy area becomes painful. His skin is tight, dry and shiny. In addition to this, frequent vomiting causes dehydration and imbalance of chemical elements in the blood.
The prognosis depends on how quickly the parents see a doctor, correct diagnosis and the completeness of the medical care provided. An unfavorable outcome is possible with late detected pathology or inoperable tumors. With adhesions, relapses in the future are likely.
Features of treatment of newborns and older children
If intestinal obstruction is suspected, children of any age are hospitalized in surgery. Treatment begins immediately to avoid fatal intestinal strangulation. The procedures take place in the following sequence:
- ridding the stomach and intestines of contents using a nasogastric tube;
- placing IVs to correct dehydration and electrolyte imbalances;
- in case of intestinal volvulus - correction by inserting a rectal tube (avoids surgery);
- giving infants a barium enema to combat intussusception;
- This enema can be replaced by an air enema, which copes well with partial obstruction in infants.
After the procedures, babies remain under the supervision of a doctor in the hospital for at least 2-3 days. The doctor may prescribe antispasmodic and painkillers.
Treatment of the disease cannot be delayed. The small patient should be immediately hospitalized in the surgery department. Until a complete examination by a doctor, it is not recommended to give the baby enemas, give laxatives, or perform gastric lavage.
Treatment is prescribed only after a comprehensive examination. Examinations to detect obstruction are carried out by a surgeon. If complications are detected in the baby, only surgical intervention will be prescribed.
It is performed when there are no serious complications. Treatment consists of a set of measures to remove stagnation in the intestines and combat poisoning of the body. The little patient is prescribed fasting and rest, and intensive therapy is carried out, including the following stages:
- They use a flexible umbrella that is inserted through the nasal cavity into the stomach. Thus, the upper parts of the digestive tract are freed from food stagnation, this helps stop the vomiting process;
- solutions are administered intravenously that restore the body’s water-salt balance;
- enemas are administered with hypertonic solutions, as well as siphon enemas with sodium chloride solution;
- if the child has intussusception, then within 24 hours the intussusception is straightened by introducing air into the rectum;
- prescribe painkillers and antiemetics;
- when peristalsis is strongly expressed, antispasmodic medications (no-spa) are used;
- Proserin is administered subcutaneously to stimulate intestinal function.
Operation
When conservative therapy does not have the desired effect, surgical intervention is performed. The operation is aimed at eliminating mechanical blockage, removing the affected intestine, and preventing recurrent cases of obstruction.
During the operation the following activities are carried out:
- Remove an obstacle that prevents content from moving forward. When an operation is performed on the small intestine, a resection is performed, which completely restores patency. Sometimes surgery is performed several times to correct the problem;
- All dead tissue must be removed. It is better to remove a little more of the affected tissue and exclude recurrent obstruction;
- After surgery, saline solutions are continued to be administered to restore electrolyte balance. Anti-inflammatory therapy is also carried out.
Laxative
During a mild course of the disease, in order to alleviate the symptoms in the child, it is possible to use laxatives, including those prepared independently.
In case of congenital obstruction, surgical intervention cannot be avoided - its early implementation increases the newborn’s chances of a successful outcome. Other forms of the disease can often be cured with conservative methods. For any type of obstruction, it is important to seek medical help at the very first symptoms.
Most often, the only chance to save the patient is to perform an operation, the type of which depends on the cause of the disease.
Surgical treatment of symptoms of intestinal obstruction in children is indicated if more than twelve hours have passed since the onset of initial symptoms, there is confirmation of a congenital anomaly, there is a high risk of recurrence, or a foreign body or mechanical barrier is detected. Perform the following manipulations:
- Some of the dead intestine is removed and the remaining part is stitched together.
- In case of a hernia, it is sutured and the intestine is adjusted. If the tissue is alive, then removal is not carried out.
- Straighten the loop during intestinal volvulus.
- The foreign body is removed.
After surgery, the little patient is prescribed antibacterial or anti-inflammatory medications, as well as saline solutions to stabilize the condition.
To relieve signs of intestinal obstruction in a child in the initial stage of the disease, the use of traditional medicine methods is allowed, but strictly in agreement with the treating pediatric surgeon. It is advisable to use them only in cases of partial obstruction. Self-treatment, that is, without consulting a specialist, is fraught with a threat to the baby’s health. The most popular options include:
- Fresh cucumbers, melon, pineapple, tomatoes, peaches, prunes have a laxative effect.
- The juice of one plum is diluted with water in a 1:1 ratio. Take two tablespoons before meals.
- Pumpkin porridge and puree.
- Sea buckthorn oil is added to compote or tea, and half a teaspoon is given to the child three times a day.
- Mix equal parts of pre-chopped figs, dried apricots, prunes and raisins, add a small amount of honey. Give the baby a teaspoon several times a day.
Causes of the disease
The main common causes of intestinal obstruction in children should still be mentioned. This:
- some disturbances in the functioning of internal organs;
- existing inflammatory processes;
- accidental entry of foreign objects;
- some parasites and worms;
- adhesive clusters;
- neoplasms;
- hernias;
- formation of gall and fecal stones.
It is worth considering the stages of the disease. According to medical practice, it has three stages:
- The initial stage of the disease lasts about 3-12 hours, and is usually accompanied by pain in the abdomen, severe rumbling and flatulence.
- The duration of the intermediate stage of the disease takes about 13-36 hours. The patient feels some relief, but this is just an imaginary sensation. During this period, intoxication of the child’s body and partial dehydration occur.
- Terminal is the third stage of the disease, which occurs two days after the onset of the disease. The patient's condition deteriorates sharply. All symptoms of dehydration appear, and damage to other internal organs is possible.
Classification
The main division assumes the existence of several forms of pathology, differing in etiological factor. Coprostasis happens:
- functional - a consequence of diseases of other internal organs and systems;
- organic - caused by diseases that negatively affect the intestines directly;
- allergic - influenced by individual intolerance to a particular food product;
- hypodynamic;
- medicinal;
- toxic;
- nutritional – provoked by poor nutrition (insufficient amounts of vitamins and other nutrients entering the body);
- neurogenic;
- mechanical;
- intoxication;
- proctogenic - the main cause of hemorrhoids;
- endocrine.
Separately, it is worth highlighting idiopathic coprostasis, the causes of which cannot be established.
Forms of flow:
- acute coprostasis;
- chronic.
Chapter 8
content .. 1 2 3 8 ..Congenital gastric obstruction often occurs in children in the first days of life. It can be caused by developmental anomalies of the prepyloric region or pyloric stenosis. Some of these abnormalities lead to emergencies that require urgent surgical intervention.
Malformations of the stomach, localized in its prepyloric section, are extremely rare. Gastric obstruction is usually caused by atresia and stenosis, most often of the membranous type.
According to our proposed classification, created on the basis of our own observations and published data, there are three main types of gastric anomalies: membranous (Fig. 32, a), cord-like (Fig. 32, b) and segmental aplasia of the mucous membrane (Fig. 32, c) . With all types of atresia and stenosis of the stomach, the obstacle is localized only in the mucous membrane and submucosal layer, the muscular and serous membranes retain their continuity.
The membrane can cover the lumen of the stomach completely (atresia) or partially (stenosis); on the side or in the center of the septum there can be a hole of various sizes: from a pinhole to a large one, occupying more than half of the membrane. The thickness of the latter varies from a thin sheet to a thick, slip-shaped “hypertrophied” wall, protruding into the pyloric canal of the stomach.
Histological examination of the membranes reveals an altered mucous membrane of the gastric type with a submucosal layer and muscle tissue in the form of single fibers. The thick septum has the structure of the wall of the stomach.
Clinical picture. The time and intensity of symptoms of the disease depend on the degree of stenosis of the gastric lumen, the general condition of the child, as well as the presence of concomitant diseases.
Prepyloric gastric atresia and decompensated stenosis usually appear from the first hours or days of life. The main symptom is profuse vomiting of gastric contents without bile. Due to overdistension of the stomach and irritation of its walls from frequent vomiting, a “hemorrhagic symptom” is often added (vomit the color of coffee grounds or streaked with blood and a tarry coloration of the stool - in case of stenosis). In children, meconium passes in sufficient quantities.
Frequent, repeated vomiting usually leads to exicosis with a large drop in body weight (0.25-0.3 kg/day). Upon examination, swelling of the epigastric region is revealed, which disappears after vomiting or suction of gastric contents. Upon palpation, waves of peristalsis and the contours of a distended stomach are visible, often descending below the navel.
Prepyloric stenosis may appear several days or weeks after the baby is born. The time at which symptoms occur depends on the size of the hole in the membrane. The disease begins with regurgitation without bile, which turns into vomiting. Soon the latter takes on the character of “fountain” vomiting. Body weight decreases. The stool becomes leaner. Upon examination, swelling of the epigastric region and visible peristalsis of the distended stomach are revealed.
X-ray examination is one of the main diagnostic methods. On a plain X-ray of the abdominal cavity in an upright position, a large gas bubble and fluid level are noted, corresponding to a distended stomach; there is no gas in the intestinal loops (Fig. 33). Sometimes a “silent belly” is detected - the absence of gas throughout the gastrointestinal tract. In the presence of such an x-ray picture, other research methods are usually not required. Some surgeons suggest injecting iodolipol into the stomach - with gastric atresia, protrusion of the pyloric membrane into the lumen of the duodenum is observed.
X-ray examination of children with prepyloric stenosis is of great help in diagnosis. A plain X-ray of the abdominal cavity with the child in an upright position shows a large level of fluid and a small amount of gas in the intestinal loops. In such cases, a contrast study with iodolipol is undertaken, in which a long-term retention of the latter in the stomach is detected. In recent years, the use of fibrogastrostomy has reduced and often eliminated the need for x-ray examination.
Frequent vomiting leads to disruption of water and electrolyte metabolism. Perforation of the atretic stomach is possible.
Differential diagnosis must be carried out with diseases that occur in the first days and weeks of life and are accompanied by regurgitation and vomiting that does not contain bile. First of all, this applies to malformations of the gastric outlet.
Pyloric stenosis.
It is most difficult to differentiate this anomaly from prepyloric gastric stenosis if the symptoms of the latter arose from the 2-3rd week of the child’s life. The clinical manifestations of the diseases are extremely similar. In all cases, it is necessary to perform an X-ray examination with contrast. The method of Yu. R. Levin (Fig. 34) makes it possible to identify the symptoms of “beak”, “shoulders”, “antenna” characteristic of pyloric stenosis.
Often, this study does not definitively establish the cause of gastric obstruction. In such cases, the diagnosis is made by laparotomy, during which you should be very careful and remember about this rare malformation. Otherwise, an error may occur even during the operation,
Pylorospasm.
Symptoms appear from the first days of a child’s life, so it is necessary to differentiate pyloric spasm from atresia or decompensated gastric stenosis. Persistent, numerous vomiting, causing disruption of the child’s general condition and leading to a sharp drop in body weight, is not typical for pylorospasm. In addition, the effectiveness of antispasmodic drugs indicates the functional nature of the disease.
Congenital duodenal obstruction
when the obstruction is located above the major duodenal papilla, it has a similar clinical and radiological picture. Usually the final diagnosis is made during surgery. In other types of congenital intestinal obstruction, the vomit contains bile, which makes it possible to exclude an abnormal development of the stomach.
Congenital diaphragmatic hernia of the esophagus
in some cases, it manifests itself as vomiting from the first day of the child’s life, but the vomitus usually contains bile or blood. In addition, X-ray examination with contrast helps in diagnosis, in which a diaphragmatic hernia is confirmed by the location of the stomach above the level of the diaphragm.
Treatment. Establishing a diagnosis of congenital gastric obstruction is an indication for surgery.
Preoperative preparation
for atresias and decompensated stenoses, it usually does not exceed 24 hours and is aimed at restoring homeostasis, treating aspiration pneumonia or preventing the latter (suction of gastric contents every 2-3 hours). In case of stenosis, preparation for surgery, if necessary, can be extended to several days.
Surgical intervention
performed under endotracheal anesthesia with blood transfusion. The choice of surgical method depends on the changes detected.
Membranous forms of atresia are eliminated by excision of the septum and suturing the wound of the stomach wall in the transverse direction, so as not to cause narrowing of this section as a result of possible swelling of the tissue in the pyloric section of the stomach at the site of excision of the membrane. Before suturing the pyloric wound, a thin polyethylene tube is passed through the child’s nasal passage into the stomach and then into the duodenum. The second tube is left in the stomach to suction out stagnant contents.
For cord-like and segmental atresias, the seromuscular layer of the stomach is dissected longitudinally, blind sacs of the mucous membrane are found, they are opened and stitched end-to-end over a thin catheter passed through the nasal passage into the duodenum. The wound of the seromuscular layer is sutured in the transverse direction if possible. After layer-by-layer suturing of the abdominal cavity, the epidural space is punctured, a catheter is installed to the Th3-Th4 level for subsequent blockade (3-5 days).
Postoperative treatment
is aimed at correcting impaired water-salt metabolism, restoring the functioning of the gastrointestinal tract, preventing and treating aspiration pneumonia.
For 2-3 days the child is on parenteral nutrition, which is calculated depending on the body weight, age of the patient, disturbances of water and electrolyte metabolism, the presence of combined anomalies or complications.
If during the operation the patient had a probe inserted below the anastomosis site, then after a day they begin to introduce breast milk (5-10 ml every 3 hours), increasing the amount of the latter by 10 ml per feeding daily. The tube is removed after 4-5 days and oral feeding is started. The child receives antibiotic therapy, blood transfusions, plasma, and albumin. In the presence of pneumonia, aerosol therapy is used up to 5-6 times a day, mustard plasters, physiotherapy, etc. Sutures are removed on the 10-12th day.
We consider acute forms of pyloric stenosis to be a type of clinical manifestation of this malformation in which the symptoms of the disease begin suddenly and proceed violently. Among children with pyloric stenosis operated on at the clinic of our institute, 6% had an acute stage of the disease.
Clinical picture. The time of onset of symptoms of the disease depends on the degree of narrowing of the pyloric canal and the compensatory capabilities of the body. In addition, the layering of pylorospasm plays an important role, which, apparently, is the reason that leads to the rapid onset and course of the disease. The first signs of the disease appear between the ages of several weeks and 1 month. The main symptom of the acute form of pyloric stenosis is “fountain” vomiting, which begins suddenly, in the midst of complete health. Vomit does not contain bile; its amount exceeds the amount of milk sucked during the last feeding. Often, vomit has a stagnant, sour odor, which indicates retention of gastric contents. In some cases, streaks of blood can be seen in the vomit. Sometimes quite severe stomach bleeding occurs.
Prolonged debilitating vomiting leads to a deterioration in the child’s general condition and disruption of water-salt metabolism (hypochloremia, exicosis, and sometimes hypokalemia). The acute stage of the disease is characterized by the fact that the child develops complete
gastric obstruction. Feeding becomes impossible; a few sips of milk cause vomiting. Children lose up to 0.4-0.5 kg of body weight in 1 - 2 days. The number of urinations decreases. There is stool retention or dyspeptic “hungry” stool appears. Upon admission to the department, patients with an acute form of pyloric stenosis become extremely worried, greedily grab the pacifier, but soon there is severe vomiting. If hospitalization is carried out on the 2-3rd day from the onset of the disease, then the child’s condition is severe, symptoms of exicosis are pronounced, and there is a large loss of body weight. An indicator of the serious condition of a child with pyloric stenosis is the daily loss of body weight in relation to birth weight (as a percentage). According to this classification, three forms of the disease are distinguished: mild (0-0.1%), moderate (0.2-0.3%) and severe (0.4% or more). In children with acute pyloric stenosis, body weight loss reaches 6-8%. Upon examination, the child reacts poorly to his surroundings, with a pained expression on his face. The skin is pale, the mucous membranes are bright and dry. The fontanelle sinks. Noteworthy is the swelling of the epigastric region, which decreases or disappears after vomiting. When stroking the abdominal wall or after several sips of food, you can notice waves of stomach peristalsis. Often the stomach takes on an “hourglass” shape. This symptom is a constant sign of congenital pyloric stenosis and is of great importance for establishing the diagnosis. Another symptom characteristic of pyloric stenosis - palpation of a thickened pylorus through the anterior abdominal wall - is inconsistent, since not all children can detect it, although foreign surgeons attach great importance to this sign, proposing to palpate the pylorus in the middle of the distance between the navel and the xiphoid process, slightly to the right from the midline.
If in children with the chronic form of pyloric stenosis there are moderate changes in the biochemical blood test due to a gradual increase in symptoms of the disease, then in patients with the acute form (especially with late diagnosis) there is a sharp increase in the hematocrit number, a decrease in chlorine content, metabolic alkalosis and sometimes hypokalemia . Changes in proteins and -protein fractions occur rarely. In urine tests, traces of protein and single red blood cells can be detected. Oliguria is clearly expressed.
X-ray examination of children with suspected pilostenosis is of critical diagnostic importance. First, a survey radiograph of the abdominal cavity is taken with the child in an upright position. This reveals a large gas bubble and fluid level in the distended stomach. There is little or no gas in the intestinal loops. Then they begin the contrast study. In newborns in the first days of life, iodolipol (5 ml) is used as a contrast agent, observing its passage through the gastrointestinal tract. Lack of gastric emptying for more than 24 hours indicates an obstruction in the pyloric
department If after 4 hours more than half of the contrast agent remains in the stomach, then there is severe pyloric stenosis.
In our clinic, for the examination of children older than 3-4 weeks of life with suspected pyloric stenosis, the technique of Yu. R. Levin is used. For the study, a 20-30% suspension of barium sulfate in a 10% alucose solution heated to 37 0C is used. The child does not require special preparation. The gastric contents are sucked out through a probe and 15 ml of contrast suspension is injected. After this, the probe is pulled up to the initial section of the esophagus and the remainder of barium sulfate (5 ml) is slowly poured in. At this time, an x-ray is taken with the child lying face down with the left side elevated (this helps to obtain the most favorable projection of the pyloric canal). The next picture is taken 2 hours after the administration of the contrast agent. Pyloric stenosis is characterized by symptoms of “antral beak” or “antenna” (Fig. 34, a) and “shoulders” or “brace” (Fig. 34, b), which are revealed on an x-ray taken at the time of administration of the contrast suspension. The narrowing of the antrum of the stomach is visible on a radiograph taken 2 hours after the administration of a contrast agent (Fig. 34, c), since at this time the pylorus, deformed by spastic contraction of the muscles, forms an almost right angle with the unchanged body of the stomach.
The given technique is simple, short-term, does not require special preparation and does not exclude feeding during the examination period, the radiation exposure is small (three radiographs).
Fibrogastroscopy (FGS), used in recent years, being an excellent diagnostic method, makes X-ray examination unnecessary in some cases.
Differential diagnosis of the acute form of pyloric stenosis should be carried out with pyloric spasm, gastric obstruction, congenital high intestinal obstruction, and habitual vomiting.
The greatest importance in children in the first days of life is differentiation from pyloric spasm
due to different tactics of their treatment. It should be borne in mind that with spasm, the disease begins gradually, with regurgitation, which is inconsistent in nature, without significantly affecting the general condition of the child and his body weight. In addition, the acute form of pyloric stenosis is so acute and violent that the attending physicians assume an “acute surgical disease” and refer the child to the surgical department. If an X-ray examination is performed to differentiate these conditions, then it should be taken into account that with pylorospasm, gastric emptying begins 10 minutes after taking a contrast agent and ends after 3-6 hours.
Congenital gastric obstruction
clinically and radiologically it is extremely difficult to distinguish from the acute form of pyloric stenosis. Typically, the final diagnosis is made during surgery or during FGS.
Congenital anomalies of the duodenum,
in which the obstruction is located below the major papilla, duodenum
intestines, it is usually easy to distinguish from pyloric stenosis by bile-stained vomit and a characteristic x-ray picture. In cases of duodenal obstruction, when the obstruction is located above the major duodenal papilla, diagnosis becomes difficult. It should be remembered that with congenital intestinal obstruction, vomiting usually begins from the first day of life, while with pyloric stenosis it occurs much later. Palpation determination of a thickened pylorus and the identification of lengthening and narrowing of the pyloric canal during X-ray examination speaks in favor of pyloric stenosis.
Sometimes the contrast agent (with pyloric stenosis) remaining in the stomach may appear on the radiograph as two depots located on either side of the spine, which is similar to the X-ray picture with high intestinal obstruction. In these cases, the diagnosis is helped by a lateral radiograph - the dilated duodenum is usually located posterior to the stomach.
Habitual vomiting and regurgitation are quite common in children in the first months of life, but this dysfunction of the stomach usually does not change the general condition of the child and does not cause a drop in body weight.
Treatment. The only treatment for acute pyloric stenosis is surgery.
Preoperative preparation.
The duration and intensity of preoperative preparation depend on the timing of the child’s admission to the department and the severity of his condition. Preparation for surgery, together with examination, does not exceed 24 hours and is aimed at reducing disturbances in water-salt metabolism, as well as treating aspiration pneumonia. Immediately before the operation, gastric contents are suctioned.
Endotracheal anesthesia should be considered the best method of pain relief.
Pylorotomy technique according to Fredet - Ramstedt. An upper para- or transrectal incision on the right, 3-4 cm long, or a transverse skin incision above the projection of the pyloric canal (to prevent wound dehiscence). The pyloric part of the stomach is brought into the wound, which the surgeon fixes with the fingers of his left hand. In the avascular area, the serosa and superficial layers of the pyloric muscles are longitudinally dissected (Fig. 35, a). Then, using anatomical tweezers or a grooved probe, bluntly push the muscle fibers apart until the submucosal layer of the pylorus is completely released and bulges into the wound (Fig. 35, b). Particular care must be taken when separating muscles in the distal pylorus, near the duodenum. It is in this place that injuries to the mucous membrane most often occur due to the fact that the duodenum here forms a fold extending into the area of the pylorus (Fig. 35, c).
To prevent this complication, the pyloric tissue should be divided in the direction from the duodenum to the pylorus. In this case, the instrument will not enter the danger zone—the fold of the mucous membrane at the junction of the pylorus and the duodenum.
Bleeding from a pyloric wound is rare, but when it occurs, it is necessary to trim the bleeding vessels with an atraumatic needle. Before immersing the stomach into the abdominal cavity, the integrity of the mucous membrane is checked by pressing on the stomach and moving gas into the duodenum. When the mucous membrane is perforated, gas bubbles or a drop of gastric contents appear in the wound. The complication is dangerous only in unidentified cases. In this case, it is inappropriate to limit oneself to suturing the mucous membrane or suturing the omentum to the site of perforation, which usually does not create complete tightness and leads to peritonitis in the postoperative period.
Surgical technique for damage to the mucous membrane during pylorotomy. Using an atraumatic needle, the hole in the gastric mucosa is carefully sutured with interrupted sutures (Fig. 36, a), then the muscles and serosa of the pylorus are sutured in layers along the entire length of the surgical incision. Departing from the line of the formed sutures by 0.7-0.8 cm, the most avascular area is again selected and the pylorotomy is performed again (Fig. 36, b), avoiding mistakes made during the previous intervention.
The stomach is immersed in the abdominal cavity. The wound is sutured tightly in layers after administration of an antibiotic solution. In cases of injury to the gastric mucosa, nipple drainage is left in the abdominal cavity for 3-4 days for daily administration of antibiotics.
Postoperative treatment.
3-4 hours after the operation, if there is no injury to the mucous membrane of the stomach or duodenum, the child is given 7-10 ml of 5% glucose solution through the nipple, after 1 hour-10 ml of expressed breast milk, and then, in the absence of vomiting, is prescribed every 2 hours 10 ml of milk. Subsequently, 100 ml of milk per day is added daily. After 7-10 days, the baby is put to the breast and transferred to 7 feedings a day. If the duodenal mucosa is damaged, feeding begins no earlier than 24 hours after surgery. If the child continues to vomit, then the amount of milk is slightly reduced and a 1% solution of novocaine is prescribed, 1 teaspoon 3 times a day. The missing amount of fluid and salts is replenished parenterally, taking into account comparative data from blood tests, the child’s body weight, and his condition.
In case of aspiration pneumonia, active therapy started in the preoperative period is continued. To prevent wound infection and complications, antibiotics are used (6-7 days). Vitamin therapy is prescribed. Sutures are removed 10-12 days after surgery.
content .. 1 2 3 8 ..
Symptoms
The disease is distinguished by the fact that it has its own specific clinical picture, which is why an experienced specialist has virtually no problems establishing the correct diagnosis.
The most characteristic symptoms of the pathological syndrome are:
- rare urge to defecate - the minimum duration of constipation can be 3 days;
- change in the consistency of feces - feces become dry and hard, which provokes pain in the anal area;
- the need to push hard so that a small amount of dense and spherical feces comes out;
- heaviness and fullness of the intestines;
- paroxysmal nausea, which in rare cases causes vomiting;
- abnormal heart rate;
- loss of appetite or complete aversion to food;
- sleep disorders;
- an increase in the size of the anterior wall of the abdominal cavity;
- excessive release of gases;
- frequent mood swings;
- rumbling and severe pain in the abdomen;
- decreased ability to work;
- pale skin;
- the presence of blood impurities in the stool.
All clinical manifestations of the disease are typical for both adults and children; only the degree of severity of symptoms may differ.
Intestinal obstruction in a child
If there is a slowdown in the process of fecal excretion or its complete cessation, doctors say that intestinal obstruction in children has been diagnosed. The disease is complex and multi-causal.
The disorder is caused by congenital malformations of the intestinal region, motor dysfunction of the organ, and growing tumors. The pathology requires immediate medical intervention, because...
there is a high risk of developing severe consequences, including the death of a child or newborn. The disease is treated with medication, diet therapy, and surgery.
Description of the pathology
Intestinal obstruction in children is a pathology associated with a failure in the process of pushing chyme (broken down food with digestive juice) through the lumen.
In babies of the first year of life, the disease is accompanied by severe pain, cramps, and vomiting. Most people use surgical tactics to eliminate pathology, especially in newborns.
Older children are prescribed conservative treatment and diet.
In infants, the disease causes severe cramping pain.
Children's intestinal obstruction is a kind of blockage of the lumen. The complexity and severity of the disease depends on the location of the problem - the higher the blockage occurs, the more severe the disease will be.
The peculiarity is the manifestation of specifically rapid symptoms in a vivid form. Correct and timely response in the form of treatment determines the outcome.
If the chronic form is eliminated with medication, then the acute form can only be eliminated surgically.
Classification of intestinal obstruction in children
Intestinal obstruction in newborns and older patients is classified according to genetics, anatomical-physiological, and symptomatic parameters. Correctly determining the type of blockage allows you to prescribe adequate treatment and adjust the intensity of the measures taken. International classification:
- Based on origin, a distinction is made between congenital and acquired forms.
- According to the mechanism of formation - mechanical, dynamic.
- According to the characteristics of the symptoms - complete, partial, acute, chronic.
- According to the nature of compression of the vessels supplying the intestine with blood - strangulation, obstruction, mixed (with adhesions).
Congenital
The formation of intestinal obstruction can begin in the womb.
This form of intestinal obstruction is formed in the womb against the background of fetal development abnormalities, so the newborn suffers from severe symptoms of dysfunction from the first hours.
When the disease is particularly severe, the baby develops vomiting of bile and bloating. In mild forms of the disease, constipation and vomiting are observed. If this pathology is detected late, the risk of intestinal rupture increases.
Manifestations of congenital pathology are stenosis (narrowing of blood vessels, lumen), atresia (fusion of organ walls), and inflammation. This form is typical for newborns.
Acquired
Pathology is provoked by external or internal unfavorable factors. It most often develops in infants aged from 4 months to a year in the form of intussusception (penetration of one part of the intestine from another) or a mechanical disorder.
Adhesions are formed quite rarely. The characteristic features of the disease are an unexpected, paroxysmal pain syndrome that progresses to vomiting, and blood and mucus are found in the stool.
A childhood illness requires immediate hospitalization of the baby.
The main cause of obstruction is stagnation of feces against the background of weakness (atony) of the intestinal muscles, and, consequently, peristalsis.
Dynamic
Jumps in intestinal pressure provoke peritonitis.
The development of this form is provoked by weakening of the regional blood supply to the mesentery, disruption of water and electrolyte balance, and dysfunction of the central nervous system departments responsible for correcting the functioning of the gastrointestinal tract. As a result, inflammation develops. The incidence is 10% of all recorded cases. Classification into subforms:
- paralytic, when the problem of atony arises against the background of the operation and is accompanied by paresis, a jump in intraintestinal pressure, which is fraught with intestinal rupture and peritonitis;
- spastic pathologies, characterized by excessive muscle tension, paroxysmal abdominal pain, absence of a jump in temperature, bloating, but vomiting is possible.
Mechanical
This pathology can be caused by the formation of adhesions in the body against the background of improper wound healing after intervention in the abdominal cavity. Depending on the causative factors, there are the following subforms:
- adhesive, formed against the background of adhesion;
- obstructive, formed when the intestinal lumen is compressed by tumor tissue, foreign bodies, parasites, or blockages with food bolus, but without compression of the mesenteric vessels.
Stage-by-stage development
The onset of the disease is characterized by strong rumbling in the abdomen.
Intestinal obstruction in newborns and older children develops in 3 stages:
- The first, initial stage lasts 3-12 hours. Characteristic symptoms are abdominal pain, strong rumbling, flatulence.
- The intermediate stage is 13-36 hours. During this period, the baby shows signs of imaginary improvement, which characterizes the beginning of intoxication of the body with partial loss of fluid.
- The last, terminal stage overtakes the baby with a sharp increase in symptoms and damage to other organs.
Causes
Common provocateurs for the development of childhood intestinal obstruction are the following disorders and conditions:
- dysfunction of some internal organs (congenital and acquired);
- inflammatory processes;
- foreign bodies, parasites, worms;
- formation of a large number of adhesions;
- tumors of various nature, hernias;
- formation of stones from bile and feces.
Revealing
If you notice the first symptoms of the disease in a child, you should immediately seek medical help, because in the case of an acute course, late diagnosis is fraught with complications and even the death of the baby.
The diagnostic tactics used by the doctor are as follows:
- Questioning, examination, palpation of the child’s abdomen to identify the clinical picture.
- X-ray examination. It can be carried out with barium contrast, air injection - to determine the places of narrowing, fusion, shortening or lengthening of the sigma.
- Laparoscopy. Used in emergency cases - intestinal volvulus, adhesive obstruction.
- Ultrasound is an auxiliary examination method.
Conservative technique
It is used in standard cases of intestinal obstruction in children and infants. The objectives of the course are to eliminate congestion in the intestines and stop the process of intoxication in the body. The baby will have to fast in complete rest for some time. The stages of intensive treatment are as follows:
- use of a nasogastric tube to clear the upper gastrointestinal tract and stop vomiting;
- intravenous infusion of solutions to restore water-salt balance;
- administration of hypertensive and siphon enemas;
- straightening the intestine by introducing air in case of confluence of one intestinal section into another;
- taking painkillers, antiemetics, antispasmodics, for example, “No-shpa”;
- subcutaneous administration of “Proserin” to stimulate intestinal function;
- further diet therapy with a menu excluding irritating foods.
Surgical intervention
Surgery is used in complex cases and when conservative treatment is ineffective. The objectives are to remove the cause of the blockage and prevent relapse. Stages:
- elimination of the site of pathological narrowing (repetition may be required);
- excision of all dead tissue on the intestine with the capture of a piece of adjacent healthy tissue.
Laxatives
Drugs in this group are prescribed for mild intestinal obstruction or when there are no complications in the baby. Medications are indicated to alleviate the clinical picture.
You can buy them at the pharmacy chain or prepare them yourself.
Below are the most popular: plum juice 1:1 with water (indicated regardless of age), “Maltsupex” (maltose and barley extract soften the stool, after the condition normalizes, the dose is reduced), glycerin suppositories.
Source: https://PishcheVarenie.ru/tolstaja-kishka/neprohodymost/u-detej.html
Diagnostics
Often, no problems arise in establishing a final diagnosis, but it is much more difficult to find out why a person has developed coprostasis. The diagnostic process will include a whole range of activities.
A specialist in the field of gastroenterology must personally carry out several activities:
- get acquainted with the medical history - in some cases this will allow you to accurately determine which pathological factor provoked stagnation of feces in the terminal intestine;
- collect a life history - information regarding a person’s eating habits, medications and lifestyle;
- tapping and palpating the anterior wall of the peritoneum;
- digital examination of the rectum;
- a detailed survey of the patient - to determine the severity of characteristic clinical manifestations.
Additional laboratory and instrumental examinations involve the following procedures:
- general clinical blood and urine tests;
- blood chemistry;
- PCR tests;
- coprography;
- ultrasonography of the gastrointestinal tract;
- irrigoscopy of the large intestine;
- EFGDS;
- CT;
- MRI;
- endoscopic biopsy;
- sigmoidoscopy;
- colonoscopy;
- anorectal manometry;
- sphincterometry.

Sphincterometer
However, in some cases, such measures are not enough; consultation with specialists from other fields of medicine may be required.
Congenital low intestinal obstruction
DIAGNOSTIC METHODS, APPROACHES AND PROCEDURES [1-3]
Diagnostic criteria [1-3]
In the prenatal period:
Complaints and anamnesis: presence in the family of children with developmental defects and chromosomal abnormalities.
Laboratory tests: no specific tests.
NB ! When antenatally diagnosing intestinal obstruction, cystic fibrosis should be excluded. For this purpose (if possible), the blood of both future parents and the fetus is tested for the presence of the cystic fibrosis gene. If both parents are heterozygous for the cystic fibrosis gene, then the birth of a sick child is very likely, and in this case it is advisable to recommend termination of pregnancy; In the blood of a pregnant woman, an increase in the level of alpha-fetoprotein may accompany.
Instrumental studies [4-7]:
· Ultrasound of the fetus – atresia of the small and large intestines – at 20-24-29 weeks. – division (expansion) of intestinal loops at different levels (many dilated intestinal loops) with increased peristalsis and floating meconium particles, the number of loops reflects the level of obstruction.
NB ! Prenatal consultation: The consultation should include a geneticist, an ultrasound diagnostic doctor, an obstetrician-gynecologist, a neonatal surgeon, and, if indicated, a neonatologist and other specialists. During the consultation, the pregnant woman and her family members are informed about the nature of the damage to the fetus, possible pregnancy outcomes, and the prognosis for the life and health of the child. If indicated, recommendations are given regarding termination of pregnancy.
AFTER BIRTH:
If intestinal obstruction was diagnosed antenatally, immediately after the birth of the child it is necessary to install a gastric tube and empty the stomach, and transfer the newborn to a specialized hospital
Complaints and anamnesis:
· the earliest and most constant symptom is the absence of meconium: - with stenosis and complete atresia of the intestine, meconium is excreted in small portions and during a cleansing enema, only casts of uncolored mucus are obtained; - with volvulus, meconium and transitional stool can be excreted until the 4-5th day of life, then the stool becomes scanty with an admixture of blood, and, finally, its excretion stops. · Vomiting: you should pay attention to the time of its appearance, the intensity of its manifestation, the presence of pathological impurities in the vomit, the connection of vomiting with feeding (vomiting “fountain”, regurgitation, regurgitation) , the dynamics of this symptom. The nature of the vomit (regurgitated) masses varies depending on the level at which the obstruction of the intestinal tube occurred. In newborns with intestinal obstruction syndrome, which develops at the level of the jejunum, ileum and colon, vomiting of chyme, including feces, occurs. · Abdominal pain - in newborns can be judged by their behavior: the child becomes restless, kicks his legs. Attacks of anxiety indicate cramping pain characteristic of strangulation obstruction (midgut volvulus, Ladd syndrome, ileal volvulus). Overstretching of the intestinal loops with low atresia also causes abdominal pain, which intensifies with palpation, while the child groans. By the end of the first day of life, the child’s condition gradually worsens: he is worried, his cry becomes painful. The phenomena of intoxication are rapidly increasing - lethargy, adynamia, microcirculation disturbance. The abdomen is progressively swollen, due to overstretching of the intestinal loops, which compete through the anterior abdominal wall, peristaltic waves can be observed · Intoxication and exicosis increase rapidly due to overstretching of the intestinal loops, impaired permeability of the small intestine, and absorption of toxins by the peritoneal layers.
Instrumental studies :
· X-ray examination of the abdominal cavity - a survey X-ray of the abdominal cavity in a vertical position. With low intestinal obstruction, plain radiographs can reveal increased gas filling of intestinal loops, dilated loops, and sometimes the presence of levels.
· Irrigography (the study is carried out with a water-soluble contrast agent introduced through the rectum), in which:
- in case of obstruction, a sharply narrowed colon is contrasted; - a very high standing of the cecum - with Ledd's syndrome; - a very low standing of the cecum - with the acute form of Hirschsprung's disease; - a sharp and low-lying right bend is characteristic of low atresia, blunt and high-lying - for Hirschsprung's disease.
· X-ray contrast study (water-soluble contrast): a contrast mark is passed through the gastrointestinal tract with X-ray control (after 30 minutes, 1 hour, 3 hours, 6 hours, 12 hours).
With malrotation syndrome: delayed evacuation from the dilated duodenum, the duodenum-small intestinal junction is located to the right of the spinal column and can be identified by the “beak” symptom - contrast from the duodenum, entering the volvulus zone, looks like a thin “beak” tapering towards the end.
Ultrasound of the abdominal organs (Doppler): for malrotation syndrome (volvulus of the midgut):
– abnormal location and pulsation of the superior mesenteric vein, which normally lies central and to the right of the superior mesenteric artery; - “snail” symptom (the tortuous course of the mesenteric vessels in the volvulus leg).
Indications for specialist consultation:
· consultation with a neurologist - if changes in the central nervous system are detected (hydrocephalus, ventriculomegaly, hypoxic - ischemic brain damage) on the NSG or with a combination of malformations of the central nervous system; · consultation with a cardiologist - prescription of conservative therapy if hemodynamic disorders are detected; · consultation with a urologist – determining the timing of pathology corrections when identifying pathologies of the genitourinary system; · consultation with a geneticist – to identify chromosomal abnormalities.
Diagnostic algorithm:
Source: https://diseases.medelement.com/disease/%D0%B2%D1%80%D0%BE%D0%B6%D0%B4%D0%B5%D0%BD%D0%BD%D0%B0 %D1%8F-%D0%BD%D0%B8%D0%B7%D0%BA%D0%B0%D1%8F-%D0%BA%D0%B8%D1%88%D0%B5%D1%87 %D0%BD%D0%B0%D1%8F-%D0%BD%D0%B5%D0%BF%D1%80%D0%BE%D1%85%D0%BE%D0%B4%D0%B8% D0%BC%D0%BE%D1%81%D1%82%D1%8C-2017/15646
Treatment
After a final diagnosis is made, conservative therapeutic methods are turned to, among which the most effective are:
- diet therapy - the diet is compiled individually, depending on the etiological factor;
- taking medications must be individual;
- use of rectal suppositories with a laxative effect;
- performing cleansing enemas;
- therapeutic massage course;
- specially designed gymnastic exercises;
- traditional recipes - patients are allowed to use only after the approval of the attending physician.
If a month after the start of treatment the methods do not show a positive result, there is a need for surgical intervention. During the operation, the fecal stone and the intestinal wall where the calculus was attached can be excised.
Causes
Experts suggest that the main causes of dynamic intestinal obstruction are disturbances in the excitability of certain nervous systems or blood circulation. The following factors may predispose to the development of these conditions:
- peritonitis and other acute inflammatory processes (for example, acute pancreatitis, appendicitis);
- abdominal injuries with hemorrhages into the mesentery;
- complicated course of chronic pathologies of the digestive system;
- blockage of blood vessels;
- consequences after surgical interventions;
- fractures of the spine or pelvis;
- CNS lesions: traumatic brain and spinal cord injuries, ischemic stroke, mental trauma, uremia, etc.;
- acute mesenteric infarction;
- acute intoxication: poisoning with heavy metal salts, intestinal infections, food intoxication;
- complicated course of certain diseases of the chest and abdominal organs (for example, myocardial infarction, urolithiasis, pleurisy, etc.).
Treatment of constipation in children
The chronic form of coprostasis is not considered a dangerous condition for humans, but often causes complications. The longer the delay lasts, the more serious the consequences. If treatment for constipation is not started in time, complications may develop:
- fissures in the anus;
- volvulus;
- haemorrhoids;
- loss of appetite;
- depression;
- intoxication of the body;
- expansion of the sphincter muscles;
- internal bleeding;
- deformation of the rectum.
In a child’s body, pathology also provokes a decrease in the absorption of vitamins necessary for a growing body. To avoid negative consequences, you need to start comprehensive treatment of the pathology. Effective therapy includes:
- adherence to daily routine;
- diet;
- Exercise therapy (physical therapy);
- taking medications (only as prescribed by a doctor);
- physiotherapy;
- use of folk remedies.










