Structure and topography of the esophagus
The esophagus begins at the level of the VI cervical vertebra with a formation called the entrance to the esophagus
, and ends at the level of the left edge of the body of the X or XI thoracic vertebrae with a formation called
cardia
. The wall of the esophagus consists of adventitia, muscular, submucosal layers and mucous membrane (Fig. 1).
Rice . 1.
Layers of the esophageal wall (according to Kupriyanov P.A., 1962): a - cross-section of the esophagus; b — longitudinal section of the esophagus; 1 - muscle layer; 2, 5 — mucous membrane; 3 - own muscular layer of the mucous membrane; 4.7 - submucosal layer; 6 - muscle layer
The muscles of the esophagus consist of an outer longitudinal and an inner circular layer. The intermuscular autonomic plexus is located in the esophagus. In the upper third of the esophagus there is striated muscle, in the lower third there is smooth muscle; in the middle part there is a gradual replacement of striated smooth muscle fibers. When the esophagus passes into the stomach, the inner muscular layer forms the cardiac sphincter
. When it spasms, obstruction of the esophagus can occur; when vomiting, the sphincter gapes.
The esophagus is divided into three topographic-anatomical sections: cervical, thoracic and abdominal
(Fig. 2).
Rice. 2.
Sections of the esophagus, front view: 1 - laryngopharynx; 2 - upper narrowing; 3 - middle (aortic) narrowing; 4 - lower (diaphragmatic) narrowing; 5 - cardiac part; 6 - abdominal part; 7 - cervical region; 8 - thoracic region; 9 - diaphragm
Cervical
, or
laryngeal, section of the esophagus
(7), 5-6 cm long, located at the level of the VI and VII cervical vertebrae behind and slightly to the left of the initial part of the trachea.
Here the esophagus comes into contact with the thyroid gland. In this section behind the esophagus there is a post-esophageal space filled with loose fiber that extends into the mediastinum, providing the esophagus with physiological mobility. The unity of the retropharyngeal, postesophageal and mediastinal spaces contributes to the emergence of generalized inflammatory processes spreading from the pharynx to the retropharyngeal space and further down into the mediastinum. In the cervical esophagus, the right recurrent nerve
.
Thoracic esophagus
(8) extends from the upper opening of the chest to the diaphragmatic opening and is equal to 17-19 cm. Here the esophagus is in contact with the aorta, main bronchi and recurrent nerves.
Before the entrance to the diaphragmatic opening at the level of the VII thoracic vertebra and up to the diaphragm, the esophagus is covered on the right and behind with pleura, therefore, with esophagitis that occurs in the lower parts of the esophagus, right-sided pleural and pulmonary complications are most often observed.
Abdominal
(6) is the shortest (4 cm), since it immediately passes into the stomach. The subphrenic part of the esophagus is covered in front by the peritoneum, which affects the clinical course of esophagitis in this area: irritation of the peritoneum, peritonitis, protective tension of the abdominal wall muscles (defense), etc.
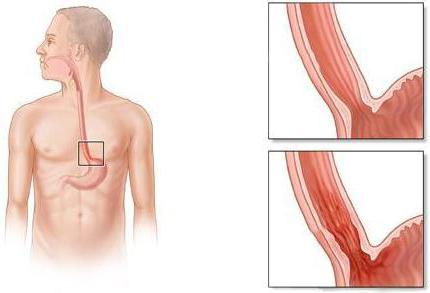
Physiological narrowing of the esophagus is of great clinical importance
, since it is at their level that foreign bodies most often get stuck and food blockages occur during functional spasm or cicatricial stenosis. These narrowings are also present at the ends of the esophagus.
Upper narrowing
(see Fig. 2,
2
) is formed as a result of spontaneous tone
of the cricopharyngeal muscle
, which pulls the cricoid cartilage to the spine, forming a kind of sphincter. In an adult, the upper narrowing of the esophagus is located at a distance of 16 cm from the upper anterior incisors.
Medium narrowing
(3) located at the intersection of the esophagus, the aorta and the left bronchus. It is located at a distance of 25 cm from the front upper incisors.
Lower narrowing
(4) corresponds to the diaphragmatic opening of the esophagus. The muscular walls of the esophagus, located at the level of this opening, function like a sphincter, opening when a bolus of food passes and closing after food enters the stomach. The distance from the diaphragmatic narrowing of the esophagus to the upper anterior incisors is 36 cm.
In children, the upper end of the esophagus is located quite high and is located at the level of the V cervical vertebra, and in old people it drops to the level of the I thoracic vertebra. The length of the esophagus in an adult varies between 26-28 cm, in children - from 8 to 20 cm.
The transverse dimensions of the esophagus depend on the age of the person. In the cervical region, its clearance in the anteroposterior direction is 17 mm, in the transverse dimension - 23 mm. In the thoracic region, the internal dimensions of the esophagus are: transverse size - from 28 to 23 mm, in the anteroposterior direction - from 21 to 17-19 mm. In the 3rd, diaphragmatic narrowing, the transverse size of the esophagus decreases to 16-19 mm, and under the diaphragm it increases again to 30 mm, forming a kind of ampulla (ampulla oesophagei). In a 7-year-old child, the internal size of the esophagus ranges from 7-12 mm.
Blood supply to the esophagus
.
In the cervical esophagus, the sources of blood supply are the upper esophageal arteries, the left subclavian artery
and a number of esophageal arterial branches arising from
the bronchial arteries
or from
the thoracic aorta
.
Venous system of the esophagus
represented by a complex venous plexus.
The outflow of blood occurs in ascending and descending directions through the veins accompanying the arteries of the esophagus. These venous systems are interconnected through portocaval esophageal anastomoses
. This is of great clinical importance when there is a blockage of venous outflow in the portal vein system, resulting in varicose veins of the esophagus, complicated by bleeding. In the upper part of the esophagus, varicose veins can be observed with malignant goiter.
Lymphatic system of the esophagus
clinically, it determines the development of many pathological processes both in the esophagus itself and in periesophageal formations (metastasis, spread of infection, lymphostatic processes). The outflow of lymph from the esophagus occurs either towards the lymph nodes of the perigastric region or to the lymph nodes of the pharynx. The indicated directions of lymphatic drainage determine the areas of spread of metastases in malignant tumors of the esophagus, as well as the spread of infection in the event of damage to it.
Innervation of the esophagus
.
The esophagus receives autonomic nerve fibers from the vagus nerves
and
borderline sympathetic trunks
.
the recurrent nerves
approach the esophagus , below from the vagus nerves, forming
the anterior
and
posterior superficial esophageal parasympathetic plexuses
.
The nerves branching out from the superior border sympathetic trunks
. The listed nerve systems innervate the smooth muscles of the esophagus and its glandular apparatus. It has been established that the mucous membrane of the esophagus has temperature, pain and tactile sensitivity, and to the greatest extent at the junction with the stomach.
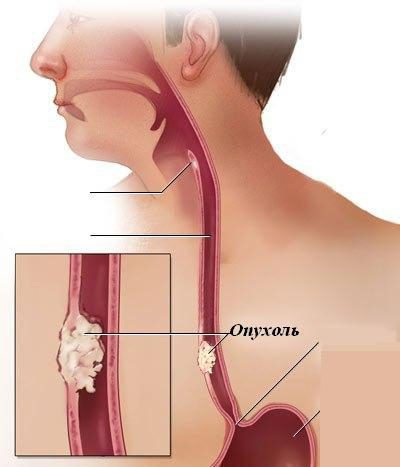
Characteristic symptoms
A sign of stenosis is primarily a violation of the swallowing process.
Other indirect symptoms indicating narrowing of the esophagus:
- Regurgitation of uncurdled milk by newborns. If the milk does not curdle, it means that it could not enter the stomach. Congenital narrowing of the esophagus can already appear during the introduction of complementary foods containing solid particles. In this case, the baby refuses food, often burps, and has a gag reflex.
- In older adults, chest pain occurs due to tension in the muscles of the esophagus when trying to push food through the narrowing site, further into the stomach.
- Increased salivation (hypersalivation) is a reaction to food masses that accumulate in the esophagus, unable to pass further into the stomach.
- Nausea and vomiting.
- Discharge of large amounts of mucus from the nose.
- Sudden weight loss caused by indigestion, the inability of food to pass through the esophagus and enter the stomach. With this condition, vitamin deficiency develops. In severe cases, cachexia (depletion of the body) may develop.
Stenosis can be complicated by pneumonia. Often with this pathology, pieces of food get into the respiratory tract. As a result of this disease, serious inflammation of the esophagus can develop and even rupture with bleeding. Such complications require urgent medical intervention.
Physiological functions of the esophagus
The movement of food through the esophagus is the last phase in the complex mechanism that organizes the entry of the bolus of food into the stomach. The act of food passing through the esophagus is an active physiological phase that occurs with certain interruptions and begins with the opening of the entrance to the esophagus. Before the opening of the esophagus, there is a short period of delay in the act of swallowing, when the entrance to the esophagus is closed, and the pressure in the lower part of the pharynx increases. At the moment of opening of the esophagus, the food bolus is directed under pressure to its entrance and slips into the reflexogenic zone of the upper part of the esophagus, in which peristalsis of its muscular apparatus occurs.
The entrance to the esophagus opens as a result of relaxation of the pharyngo-cricoid muscle. As the food bolus approaches the cardia, the diaphragmatic opening of the esophagus also opens, partly reflexively, partly as a result of the pressure that the esophagus exerts on the food bolus in its lower third.
The speed at which food moves through the esophagus depends on its consistency. The movement of food is not smooth, but is slowed down or interrupted by stops as a result of the occurrence of zones of muscle contraction and relaxation. Typically, dense products are delayed for 0.25-0.5 s in the area of aortobronchial constriction, after which they are further advanced by the force of a peristaltic wave. Clinically, this narrowing is characterized by the fact that it is at its level that foreign bodies are more often retained, and with chemical burns, deeper damage to the walls of the esophagus occurs.
The muscular system of the esophagus is under constant tonic influence of the nervous sympathetic system. It is believed that the physiological significance of muscle tone lies in the tight coverage of the food bolus by the wall of the esophagus, which prevents air from entering the esophagus and entering the stomach. Violation of this tone leads to the phenomenon of aerophagia
- swallowing air, accompanied by swelling of the esophagus and stomach, belching, pain and heaviness in the epigastric region.
Reviews
Dear readers, your opinion is very important to us - therefore we will be glad to hear your feedback about terminal esophagitis in the comments, this will also be useful to other users of the site.

Olga:
Terminal esophagitis occurs against the background of other diseases. Therefore, in order to eliminate it, it is necessary to identify the cause. You can try to do something yourself to prevent the disease from developing. I never lie down after eating, sleep on high pillows, try not to lie down for long, and, of course, I stick to my diet. Only thanks to this I was able to completely eliminate the manifestations of the disease without taking any medications.
Svetlana:
As far as I know, chronic manifestations of terminal esophagitis have to be dealt with throughout life. It is necessary to eat properly, especially during periods of exacerbation. Even the slightest deviations in the diet will negate all previous efforts.
Treatment of pathology
What treatment methods are recommended for patients diagnosed with narrowing of the esophagus? Treatment of pathology is the expansion of the damaged area.
It is important not to forget about your diet. Until recovery occurs, you need to eat only liquid and semi-liquid foods.
If peptic stricture of the esophagus is observed, the patient is prescribed antacids and astringents.
However, conservative therapy rarely leads to complete recovery. Most often it is prescribed to prepare the patient for surgery.
Bougienage (artificial dilation using special devices) is used if a benign tumor of the esophagus is detected. During the treatment, the size of the bougie is gradually changed to a larger one.
If complications occur, a gastrostomy tube is placed to provide patients with normal nutrition.
Esophagoplasty is the transplantation of a section of the intestine or stomach into the esophagus.
In severe cases, when the body is very exhausted, or surgery is not possible, gastrostomy is performed. In this case, the body is able to feed enterally.